Prostate Biopsy
|
|
Click "Control + F" to search this page only
(collapsible topics info compiled at bottom of page) |
This section gives background information about prostate biopsy. Please see Prostate Biopsy Procedure for procedural aspect.
Complications:
COMPLICATIONS
TRUS prostate post biopsy complication include urinary tract infection, emergency department presentations (0%-6%), hospitalization (up to 4%), and severe sepsis of 0%-1% is observed. 30 day mortality estimates are 0.1% up to 1. Risk factors for post biopsy infectious complications include recent hospital admission, being a hospital worker or relatives of hospital workers, recent international travel, bacteruria. Diabetes, cardiac valve replacement, COPD are also risk factors. (8) Independent predictors of infection include the number of cores taken and fluoroquinolone (FQ) resistant rectal vault flora. (1,4,5)
Biopsy Related Infections:
TRUS vs. PERINEAL
Transperineal prostate biopsies have lower rates of infection. Reports suggest zero or near-zero sepsis rates with trans perineal approach (9,10) and 3 larger studies totaling 8093 patients with 1 case of urosepsis reported and recent meta-analysis estimate showing rate of 0.1% urosepsis. (11,12,13,14) Transperineal biopsy is also associated with higher rates of urinary retention (14)
POST BIOPSY INFECTION TREATMENT
TREATMENT OF INFECTION
Post biopsy sepsis should be treated with carbopenems or piperacilin-tazobactam. 3rd generation cephalosporins, amoxicillin, fluroquinolones or gentamicin have a high rate of resistance in this context. (8) Amikacin (with a beta-lactam agent) can be considered, this is likely better than gentamicin (17) and some evidence suggests prophylaxis use reduces post TRUS prostate infections. (9)
PREVENTION OF INFECTION
ANTIBIOTICS
A large systemic review found prophylactic antibiotics significantly reduced the rates of bacteriuria (14.8% vs. 3.9%); bacteremia (8.6% vs. 2.1%); fever (10.8% vs. 4.0%); urinary tract infection (UTI) (9.0% vs. 3.3%); and hospitalization (3.3% vs. 0.3%). 1 versus 3 days ABX shows significant difference in bacteruria only and no difference in IV vs. PO ABX. (18) Another found a 55% reduction in PBI's if given 24hrs before vs. immediately prior to. (7) A 2020 systematic reveiw and meta-analysis found improved results with non-fluoroquinolones, longer courses and targeted therapy. (37)
RECTAL ENEMAS
Rectal enema possibly reduces rectal microbial load and also allows better visualization of the prostat. A Cochrane Review found that enemas plus antibiotics are associated with lower bacteremia rates, and no difference in bacteriuria or fever was demonstrated. (25) Some evidence suggests povidone-iodine-based enemas could reduce bacteriuria, bacteremia and the rate of PBIs, (26,27), but there is some controversy as an RCT of 865 men showed a 42% relative risk reduction, but this was not statistically significant (28) and a large systemic review found pre-biopsy enemas made no difference. (18)
DIPPING NEEDLE IN FORMALIN
Dipping the biopsy need in formalin before each individual prostate biopsy is easy and experiments using formalin disinfection show no growth fluoroquinolone resistant organisms and while several studies have shown lower rates of PBI's, the results of these studies have not been statistically significant. (30,31,32) One study of 756 patients found double the rate of infections (5.2% vs. 2.3%) with all patients requiring admission without formalin use. (32)
OTHER PREVENTIONS
Povidone iodine swab of the rectum may decrease infectious rate. (8)
TIMING OF ANTIBIOTIC PROPHYLAXIS
Systemic review of 19 trials showed administration 24 h before biopsy versus administration immediately before reduced the relative risk of post-biopsy infection by 55%. Seven studies compared different durations of antibiotic prophylaxis. None showed any benefit from continuing prophylaxis beyond a single dose or a one-day regimen. (7) One study showed 1 versus 3 days ABX showed no significant difference in bacteruria only and no difference in IV vs. PO ABX. Pre biopsy enemas made no difference. (18)
ANTIBIOTICS SELECTION
PLEASE SEE THE TABLE TOWARDS BOTTOM OF PAGE
FLUOROQUINOLONE RESISTANCE
Fluoroquinolone resistance in E. coli blood stream isolates are around 12% in US and higher in other locations. Some studies have shown targeted therapy decreases infection rate whereas some show no difference with empiric prophylaxis. (8)
FOSFOMYCIN vs. FLUROQUINOLONE
A 2017 meta-analysis of five studies covering 3112 patients looked at fosfomycin trometamol (FT) vs.FQ including three prospective randomised trials and two retrospective studies. The relative odds of an infectious complication (OR 0.22, 95% CI 0.09–0.54) or of a more severe (Grade 2) infection (OR 0.13, 95% CI 0.07–0.26) were significantly lower in those receiving FT compared to FQ prophylaxis. A low incidence of medication-related side effects was observed. There were less observed infections due to FQ-resistant pathogens in those receiving FT prophylaxis. The authors conclude that patients who received FT prophylaxis were less likely than those who received FQ prophylaxis to develop infections overall, as well as severe and resistant infections after TRUSPB. Assessing the performance of FT in other geographic locations or in comparison to targeted prophylaxis based on risk assessment or rectal cultures is desired. (3)
ERTAPENEM
Study of 326 patients found a nonsignificant increase in carbapenem-resistant rectal flora in patients treated with ertapenem as prophylaxis for TRUSPB. (29)
FLUOROQUINOLONE RESISTANCE
Fluoroquinolone resistance in E. coli blood stream isolates are around 12% in US and higher in other locations. Some studies have shown targeted therapy decreases infection rate whereas some show no difference with empiric prophylaxis. (8)
FOSFOMYCIN vs. FLUROQUINOLONE
A 2017 meta-analysis of five studies covering 3112 patients looked at fosfomycin trometamol (FT) vs.FQ including three prospective randomised trials and two retrospective studies. The relative odds of an infectious complication (OR 0.22, 95% CI 0.09–0.54) or of a more severe (Grade 2) infection (OR 0.13, 95% CI 0.07–0.26) were significantly lower in those receiving FT compared to FQ prophylaxis. A low incidence of medication-related side effects was observed. There were less observed infections due to FQ-resistant pathogens in those receiving FT prophylaxis. The authors conclude that patients who received FT prophylaxis were less likely than those who received FQ prophylaxis to develop infections overall, as well as severe and resistant infections after TRUSPB. Assessing the performance of FT in other geographic locations or in comparison to targeted prophylaxis based on risk assessment or rectal cultures is desired. (3)
ERTAPENEM
Study of 326 patients found a nonsignificant increase in carbapenem-resistant rectal flora in patients treated with ertapenem as prophylaxis for TRUSPB. (29)
BACTERIURIA
A study of 353 men undergoing TRUSPB, of which 12 had a preoperative positive urine culture, and detected no difference in the complication rates between the groups. (23) Another study of 150 patients with 6 positive preoperative urine culture found no association between asymptomatic bacteriuria and PBIs. (24)
Quality of Biopsies:
MRI FUSION BIOPSIES
About 10% of clinically significant lesions not seen on MRI were found with systemic biopsies. (15,16) with two studies finding 16% of men with negative MRI had clinically significant prostate cancer on systemic biopsy. (20,22) A 2020 study found prostate cancer was detected in 79%, 92%, 98% and 100% of cases on the 1st, 2nd, 3rd or 4th biopsy of target lesion. (35) A meta-analysis and systematic review in 2020 found that the NPV of 90.4% when using a PSAD of 0.15. (36). Please see prostate imaging for many more details about MRI imaging and fusion biopsy.
PET FUSION BIOPSIES
A prostpective study using PET fusion prostate biopsy showed if a maximum standardized uptake value of 5.4 and maximum-to-background standardized uptake value ratio of 2 had a 100% sensitivity and a 76% specificity for Gleason 7 and 88% for Gleason 6 in the first prospective study for this PET. (21)
SATURATION BIOPSY
A prospective study from 2000-2016 of 208 consecutive patients, including 86 with a saturated and 122 with a nonsaturated lesion.
Median age 62.0 years, median PSA 7.1 ng/ml. Median number of biopsy cores per index lesion was 4 in saturated vs 2 in unsaturated. The risk category upgrade rate from systematic only, fusion only, and combined fusion and systematic biopsy results to prostatectomy was 40.9%, 23.6% and 13.8%, respectively. The risk category upgrade from combined fusion and systematic biopsy results was lower in the saturated than in the nonsaturated lesion group (7% vs 18%, p = 0.021). There was no difference in the upgrade rate based on systematic biopsy between the 2 groups. However, fusion biopsy results were significantly less upgraded in the saturated lesion group (Gleason upgrade 20.9% vs 36.9%, p = 0.014 and risk category upgrade 14% vs 30.3%, p = 0.006). The authors concluded the results demonstrated that fusion saturation biopsy of an index lesion (largest and highest PIRADS) by minimizing the impact of tumor heterogeneity. (2)
Median age 62.0 years, median PSA 7.1 ng/ml. Median number of biopsy cores per index lesion was 4 in saturated vs 2 in unsaturated. The risk category upgrade rate from systematic only, fusion only, and combined fusion and systematic biopsy results to prostatectomy was 40.9%, 23.6% and 13.8%, respectively. The risk category upgrade from combined fusion and systematic biopsy results was lower in the saturated than in the nonsaturated lesion group (7% vs 18%, p = 0.021). There was no difference in the upgrade rate based on systematic biopsy between the 2 groups. However, fusion biopsy results were significantly less upgraded in the saturated lesion group (Gleason upgrade 20.9% vs 36.9%, p = 0.014 and risk category upgrade 14% vs 30.3%, p = 0.006). The authors concluded the results demonstrated that fusion saturation biopsy of an index lesion (largest and highest PIRADS) by minimizing the impact of tumor heterogeneity. (2)
Other Interesting Studies:
NUMBER OF POSITIVE CORES
To help determine whether the number of positive cores should effect active surveillance usage, a retrospective study of 3,359 men with low risk prostate cancer who underwent radical prostatectomy between January 2000 and August 2016 was reviewed. Of the 171 cases (5.1%) with adverse pathology findings at radical prostatectomy 144 (4.3%) were upgraded to Grade Group 3 or greater, 31 (0.9%) had seminal vesicle invasion and 15 (0.4%) had lymph node involvement. Prostate specific antigen and patient age were the only predictors of adverse pathology results. There was no significant association with the number of positive cores, the total mm of cancer or the maximum percent of cancer in any core. When expanding the definition of adverse pathology to include Grade Group 2 and extraprostatic extension, the association between core features and outcome was statistically significant but clinically weak, and with no evidence of threshold effects. There is little basis for excluding patients with otherwise low risk prostate cancer on biopsy from active surveillance based on criteria such as the number of positive cores or the maximum cancer involvement of biopsy cores. (6)
DOWNGRADING
A study of 5,474 Gleason 8 biopsies showed 60% were downgraded on final pathology of post-prostatectomy and this finding is consistent with multiple other studies. (19)
inflammation on prostate biopsy
A study of 20,585 found inflammation on biopsy associated with OR of 0.455 with prostate cancer. (34)
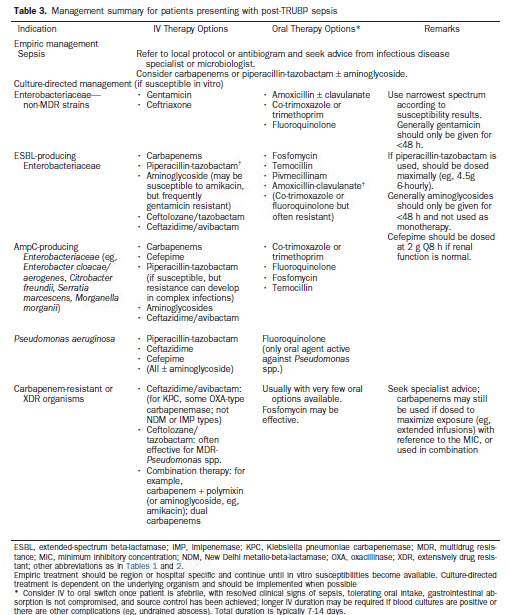
Management Strategies for Post Prostate Biopsy Infections (8)
- Papagiannopoulos, Dimitri, et al. "Predictors of infectious complications after targeted prophylaxis for prostate needle biopsy." The Journal of urology 199.1 (2018): 155-160.
- Calio, Brian P., et al. "Risk of upgrading from prostate biopsy to radical prostatectomy pathology: Does Saturation Biopsy of Index Lesion during mpMRI-TRUS fusion biopsy help?." The Journal of urology (2017).
- Roberts, Matthew J., et al. "Comparison of fosfomycin against fluoroquinolones for transrectal prostate biopsy prophylaxis: an individual patient-data meta-analysis." World journal of urology (2017): 1-8.
- Roberts, Matthew J., et al. "Baseline prevalence of antimicrobial resistance and subsequent infection following prostate biopsy using empirical or altered prophylaxis: a bias-adjusted meta-analysis." International journal of antimicrobial agents 43.4 (2014): 301-309.
- Liss, Michael A., et al. "Clinical and microbiological determinants of infection after transrectal prostate biopsy." Clinical Infectious Diseases 60.7 (2014): 979-987.
- Audenet, François, et al. "Biopsy Core Features are Poor Predictors of Adverse Pathology in Men with Grade Group 1 Prostate Cancer." The Journal of urology (2017).
- Klemann, Nina, et al. "Antibiotic prophylaxis and complications following prostate biopsies—a systematic review." Dan Med J64 (2017): A5323.
- Roberts, Matthew J., et al. "Prostate biopsy-related infection: a systematic review of risk factors, prevention strategies, and management approaches." Urology 104 (2017): 11-21.
- Loeb, Stacy, et al. "Systematic review of complications of prostate biopsy." European urology 64.6 (2013): 876-892.
- Grummet, Jeremy P., et al. "Sepsis and ‘superbugs’: should we favour the transperineal over the transrectal approach for prostate biopsy?." BJU international 114.3 (2014): 384-388.
- Namekawa, Takeshi, et al. "Prospective evaluation of the safety of transrectal ultrasound-guided transperineal prostate biopsy based on adverse events." International journal of clinical oncology 20.6 (2015): 1185-1191.
- Mai, Zhipeng, et al. "Transperineal template‐guided prostate biopsy: 10 years of experience." BJU international 117.3 (2016): 424-429.
- Pepe, Pietro, and Francesco Aragona. "Morbidity after transperineal prostate biopsy in 3000 patients undergoing 12 vs 18 vs more than 24 needle cores." Urology 81.6 (2013): 1142-1146.
- Bennett, H. Y., et al. "The global burden of major infectious complications following prostate biopsy." Epidemiology & Infection 144.8 (2016): 1784-1791.
- Borkowetz, Angelika, et al. "Comparison of systematic transrectal biopsy to transperineal magnetic resonance imaging/ultrasound‐fusion biopsy for the diagnosis of prostate cancer." BJU international 116.6 (2015): 873-879.
- Radtke, Jan Philipp, et al. "The current and future role of magnetic resonance imaging in prostate cancer detection and management." Translational andrology and urology 4.3 (2015): 326.
- Williamson, Deborah A., et al. "Escherichia coli bloodstream infection after transrectal ultrasound–guided prostate biopsy: implications of fluoroquinolone-resistant sequence type 131 as a major causative pathogen." Clinical infectious diseases54.10 (2012): 1406-1412.
- Mrkobrada, Marko, et al. "CUA Guidelines on antibiotic prophylaxis for urologic procedures." Canadian Urological Association Journal 9.1-2 (2015): 13.
- Gansler, Ted, et al. "most Gleason 8 Biopsies are Downgraded at Prostatectomy—does 4+ 4= 7?." The Journal of urology 199.3 (2018): 706-712.
- Filson, Christopher P., et al. "Prostate cancer detection with magnetic resonance‐ultrasound fusion biopsy: The role of systematic and targeted biopsies." Cancer 122.6 (2016): 884-892.
- Lopci, Egesta, et al. "68Ga-PSMA Positron Emission Tomography/Computerized Tomography for Primary Diagnosis of Prostate Cancer in Men with Contraindications to or Negative Multiparametric Magnetic Resonance Imaging: A Prospective Observational Study." The Journal of urology200.1 (2018): 95-103.
- Borofsky, Samuel, et al. "What are we missing? False-negative cancers at multiparametric MR imaging of the prostate." Radiology 286.1 (2017): 186-195.
- Bruyère, Franck, et al. "Is urine culture routinely necessary before prostate biopsy?." Prostate cancer and prostatic diseases 13.3 (2010): 260.
- Qi DZ, Lehman K, Dewan K, et al. Preoperative urine culture is unnecessary in asymptomatic men prior to prostate needle biopsy. Int Urol Nephrol 2017; 50:21–24.
- \Zani EL, Clark OA, Netto NR Jr. Antibiotic prophylaxis for transrectal prostate biopsy. Cochrane Database Syst Rev 2007; 5:CD006576.
- Allen JL, Lehman K, Dewan K, et al. Procedural povidone iodine rectal preparation reduces bacteriuria and bacteremia following prostate needle biopsy. Can J Urol 2017; 24:8883–8889.
- Gyorfi JR, Otteni C, Brown K, et al. Peri-procedural povidone-iodine rectal preparation reduces microorganism counts and infectious complications following ultrasound-guided needle biopsy of the prostate. World J Urol 2014; 32:905–909.
- AbuGhosh Z, Margolick J, Goldenberg SL, et al. A prospective randomized trial of povidone-iodine prophylactic cleansing of the rectum before transrectal ultrasound guided prostate biopsy. J Urol 2013; 189:1326–1331.
- Bloomfield MG, Page MJ, McLachlan AG, et al. Routine ertapenem prophylaxis for transrectal ultrasound guided prostate biopsy does not select for carbapenem resistant organisms: a prospective cohort study. J Urol 2017; 198:362–368.
- Issa MM, Al-Qassab UA, Hall J, et al. Formalin disinfection of biopsy needle minimizes the risk of sepsis following prostate biopsy. J Urol 2013; 190:1769–1775.
- Auffenberg GB, Qi J, Gao Y, et al. Evaluation of a needle disinfectant technique to reduce infection-related hospitalization following transrectal prostate biopsy. BJU Int 2017; 121:232–238.
- Singla N, Walker J, Woldu SL, et al. Formalin disinfection of prostate biopsy needles may reduce postbiopsy infectious complications. Prostate Cancer Prostatic Dis 2017; 20:216–220.
- Fontana, Matteo, Luca Boeri, and Emanuele Montanari. "Update on techniques to prevent infections associated with prostate needle biopsy." Current opinion in urology 28.4 (2018): 392-397.
- Vasavada, Shaleen R., et al. “Inflammation on Prostate Needle Biopsy Is Associated with Lower Prostate Cancer Risk: A Meta-Analysis.” The Journal of Urology, vol. 199, no. 5, 2017, pp. 1174–1181.
- Leyh-Bannurah, Sami-Ramzi, et al. "Minimum magnetic resonance imaging-ultrasound fusion targeted biopsy cores needed for prostate cancer detection: multivariable retrospective, lesion based analyses of patients treated with radical prostatectomy." The Journal of urology 203.2 (2020): 299-303.
- Pagniez, M. A., et al. "Predictive Factors of Missed Clinically Significant Prostate Cancers in Men with Negative Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis." The Journal of Urology (2020): 10-1097.
- Pilatz, Adrian, et al. "Antibiotic prophylaxis for the prevention of infectious complications following prostate biopsy: A Systematic Review and Meta-analysis." The Journal of Urology (2020): 10-1097.
The following text is copy pasted from the above drop down boxes, this is here so you can search control + F on this page.
BIOPSY COMPLICATIONS
TRUS prostate post biopsy complication include urinary tract infection, emergency department presentations (0%-6%), hospitalization (up to 4%), and severe sepsis of 0%-1% is observed. 30 day mortality estimates are 0.1% up to 1. Risk factors for post biopsy infectious complications include recent hospital admission, being a hospital worker or relatives of hospital workers, recent international travel, bacteruria. Diabetes, cardiac valve replacement, COPD are also risk factors. (8) Independent predictors of infection include the number of cores taken and fluoroquinolone (FQ) resistant rectal vault flora. (1,4,5)
Transperineal prostate biopsies have lower rates of infection. Reports suggest zero or near-zero sepsis rates with trans perineal approach (9,10) and 3 larger studies totaling 8093 patients with 1 case of urosepsis reported and recent meta-analysis estimate showing rate of 0.1% urosepsis. (11,12,13,14) Transperineal biopsy is also associated with higher rates of urinary retention (14)
TREATMENT OF INFECTION
Post biopsy sepsis should be treated with carbopenems or piperacilin-tazobactam. 3rd generation cephalosporins, amoxicillin, fluroquinolones or gentamicin have a high rate of resistance in this context. (8) Amikacin (with a beta-lactam agent) can be considered, this is likely better than gentamicin (17) and some evidence suggests prophylaxis use reduces post TRUS prostate infections. (9)
PREVENTION OF INFECTION
Povidone iodine swab of the rectum may decrease infectious rate. (8) A large systemic review found prophylactic antibiotics significantly reduced the rates of bacteriuria (14.8% vs. 3.9%); bacteremia (8.6% vs. 2.1%); fever (10.8% vs. 4.0%); urinary tract infection (UTI) (9.0% vs. 3.3%); and hospitalization (3.3% vs. 0.3%). 1 versus 3 days ABX shows significant difference in bacteruria only and no difference in IV vs. PO ABX. Pre biopsy enemas made no difference. (18) Another found a 55% reduction in PBI's if given 24hrs before vs. immediately prior to. (7) A 2020 systematic review found improved results with non-fluoroquinolones, longer duration and targeted therapy (37).
Rectal enema possibly reduces rectal microbial load and also allows better visualization of the prostat. A Cochrane Review found that enemas plus antibiotics are associated with lower bacteremia rates, and no difference in bacteriuria or fever was demonstrated. (25) Some evidence suggests povidone-iodine-based enemas could reduce bacteriuria, bacteremia and the rate of PBIs, (26,27), but there is some controversy as an RCT of 865 men showed a 42% relative risk reduction, but this was not statistically significant. (28)
TIMING OF ANTIBIOTICS BIOPSY
Systemic review of 19 trials showed administration 24 h before biopsy versus administration immediately before reduced the relative risk of post-biopsy infection by 55%. Seven studies compared different durations of antibiotic prophylaxis. None showed any benefit from continuing prophylaxis beyond a single dose or a one-day regimen. (7)
FLUOROQUINOLONE RESISTANCE
Fluoroquinolone resistance in E. coli blood stream isolates are around 12% in US and higher in other locations. Some studies have shown targeted therapy decreases infection rate whereas some show no difference with empiric prophylaxis. (8)
FOSFOMYCIN vs. FLUROQUINOLONE
A 2017 meta-analysis of five studies covering 3112 patients looked at fosfomycin trometamol (FT) vs.FQ including three prospective randomised trials and two retrospective studies. The relative odds of an infectious complication (OR 0.22, 95% CI 0.09–0.54) or of a more severe (Grade 2) infection (OR 0.13, 95% CI 0.07–0.26) were significantly lower in those receiving FT compared to FQ prophylaxis. A low incidence of medication-related side effects was observed. There were less observed infections due to FQ-resistant pathogens in those receiving FT prophylaxis. The authors conclude that patients who received FT prophylaxis were less likely than those who received FQ prophylaxis to develop infections overall, as well as severe and resistant infections after TRUSPB. Assessing the performance of FT in other geographic locations or in comparison to targeted prophylaxis based on risk assessment or rectal cultures is desired. (3)
BACTERIURIA
A study of 353 men undergoing TRUSPB, of which 12 had a preoperative positive urine culture, and detected no difference in the complication rates between the groups. (23) Another study of 150 patients with 6 positive preoperative urine culture found no association between asymptomatic bacteriuria and PBIs. (24)
FORMALIN DIPPING
Dipping the biopsy need in formalin before each individual prostate biopsy is easy and experiments using formalin disinfection show no growth fluoroquinolone resistant organisms and while several studies have shown lower rates of PBI's, the results of these studies have not been statistically significant. (30,31,32)
MRI FUSION BIOPSIES
About 10% of clinically significant lesions not seen on MRI were found with systemic biopsies. (15,16) with two studies finding 16% of men with negative MRI had clinically significant prostate cancer on systemic biopsy. (20,22) A 2020 study found prostate cancer was detected in 79%, 92%, 98% and 100% of cases on the 1st, 2nd, 3rd or 4th biopsy of target lesion. (35) PET FUSION BIOPSY
A prostpective study using PET fusion prostate biopsy showed if a maximum standardized uptake value of 5.4 and maximum-to-background standardized uptake value ratio of 2 had a 100% sensitivity and a 76% specificity for Gleason 7 and 88% for Gleason 6 in the first prospective study for this PET. (21) A meta-analysis and systematic review in 2020 found that the NPV of 90.4% when using a PSAD of 0.15. (36).
SATURATION BIOPSY OF TARGET
A prospective study from 2000-2016 of 208 consecutive patients, including 86 with a saturated and 122 with a nonsaturated lesion. Median age 62.0 years, median PSA 7.1 ng/ml. Median number of biopsy cores per index lesion was 4 in saturated vs 2 in unsaturated. The risk category upgrade rate from systematic only, fusion only, and combined fusion and systematic biopsy results to prostatectomy was 40.9%, 23.6% and 13.8%, respectively. The risk category upgrade from combined fusion and systematic biopsy results was lower in the saturated than in the nonsaturated lesion group (7% vs 18%, p = 0.021). There was no difference in the upgrade rate based on systematic biopsy between the 2 groups. However, fusion biopsy results were significantly less upgraded in the saturated lesion group (Gleason upgrade 20.9% vs 36.9%, p = 0.014 and risk category upgrade 14% vs 30.3%, p = 0.006). The authors concluded the results demonstrated that fusion saturation biopsy of an index lesion (largest and highest PIRADS) b by minimizing the impact of tumor heterogeneity. (2)
NUMBER OF POSITIVE CORES
To help determine whether the number of positive cores should effect active surveillance usage, a retrospective study of 3,359 men with low risk prostate cancer who underwent radical prostatectomy between January 2000 and August 2016 was reviewed. Of the 171 cases (5.1%) with adverse pathology findings at radical prostatectomy 144 (4.3%) were upgraded to Grade Group 3 or greater, 31 (0.9%) had seminal vesicle invasion and 15 (0.4%) had lymph node involvement. Prostate specific antigen and patient age were the only predictors of adverse pathology results. There was no significant association with the number of positive cores, the total mm of cancer or the maximum percent of cancer in any core. When expanding the definition of adverse pathology to include Grade Group 2 and extraprostatic extension, the association between core features and outcome was statistically significant but clinically weak, and with no evidence of threshold effects. There is little basis for excluding patients with otherwise low risk prostate cancer on biopsy from active surveillance based on criteria such as the number of positive cores or the maximum cancer involvement of biopsy cores. (6)
DOWNGRADING
A study of 5,474 Gleason 8 biopsies showed 60% were downgraded on final pathology of post-prostatectomy and this finding is consistent with multiple other studies. (19)
INFLAMMATION ON PROSTATE BIOPSY
A study of 20,585 found inflammation on biopsy associated with OR of 0.455 with prostate cancer. (34)
TRUS prostate post biopsy complication include urinary tract infection, emergency department presentations (0%-6%), hospitalization (up to 4%), and severe sepsis of 0%-1% is observed. 30 day mortality estimates are 0.1% up to 1. Risk factors for post biopsy infectious complications include recent hospital admission, being a hospital worker or relatives of hospital workers, recent international travel, bacteruria. Diabetes, cardiac valve replacement, COPD are also risk factors. (8) Independent predictors of infection include the number of cores taken and fluoroquinolone (FQ) resistant rectal vault flora. (1,4,5)
Transperineal prostate biopsies have lower rates of infection. Reports suggest zero or near-zero sepsis rates with trans perineal approach (9,10) and 3 larger studies totaling 8093 patients with 1 case of urosepsis reported and recent meta-analysis estimate showing rate of 0.1% urosepsis. (11,12,13,14) Transperineal biopsy is also associated with higher rates of urinary retention (14)
TREATMENT OF INFECTION
Post biopsy sepsis should be treated with carbopenems or piperacilin-tazobactam. 3rd generation cephalosporins, amoxicillin, fluroquinolones or gentamicin have a high rate of resistance in this context. (8) Amikacin (with a beta-lactam agent) can be considered, this is likely better than gentamicin (17) and some evidence suggests prophylaxis use reduces post TRUS prostate infections. (9)
PREVENTION OF INFECTION
Povidone iodine swab of the rectum may decrease infectious rate. (8) A large systemic review found prophylactic antibiotics significantly reduced the rates of bacteriuria (14.8% vs. 3.9%); bacteremia (8.6% vs. 2.1%); fever (10.8% vs. 4.0%); urinary tract infection (UTI) (9.0% vs. 3.3%); and hospitalization (3.3% vs. 0.3%). 1 versus 3 days ABX shows significant difference in bacteruria only and no difference in IV vs. PO ABX. Pre biopsy enemas made no difference. (18) Another found a 55% reduction in PBI's if given 24hrs before vs. immediately prior to. (7) A 2020 systematic review found improved results with non-fluoroquinolones, longer duration and targeted therapy (37).
Rectal enema possibly reduces rectal microbial load and also allows better visualization of the prostat. A Cochrane Review found that enemas plus antibiotics are associated with lower bacteremia rates, and no difference in bacteriuria or fever was demonstrated. (25) Some evidence suggests povidone-iodine-based enemas could reduce bacteriuria, bacteremia and the rate of PBIs, (26,27), but there is some controversy as an RCT of 865 men showed a 42% relative risk reduction, but this was not statistically significant. (28)
TIMING OF ANTIBIOTICS BIOPSY
Systemic review of 19 trials showed administration 24 h before biopsy versus administration immediately before reduced the relative risk of post-biopsy infection by 55%. Seven studies compared different durations of antibiotic prophylaxis. None showed any benefit from continuing prophylaxis beyond a single dose or a one-day regimen. (7)
FLUOROQUINOLONE RESISTANCE
Fluoroquinolone resistance in E. coli blood stream isolates are around 12% in US and higher in other locations. Some studies have shown targeted therapy decreases infection rate whereas some show no difference with empiric prophylaxis. (8)
FOSFOMYCIN vs. FLUROQUINOLONE
A 2017 meta-analysis of five studies covering 3112 patients looked at fosfomycin trometamol (FT) vs.FQ including three prospective randomised trials and two retrospective studies. The relative odds of an infectious complication (OR 0.22, 95% CI 0.09–0.54) or of a more severe (Grade 2) infection (OR 0.13, 95% CI 0.07–0.26) were significantly lower in those receiving FT compared to FQ prophylaxis. A low incidence of medication-related side effects was observed. There were less observed infections due to FQ-resistant pathogens in those receiving FT prophylaxis. The authors conclude that patients who received FT prophylaxis were less likely than those who received FQ prophylaxis to develop infections overall, as well as severe and resistant infections after TRUSPB. Assessing the performance of FT in other geographic locations or in comparison to targeted prophylaxis based on risk assessment or rectal cultures is desired. (3)
BACTERIURIA
A study of 353 men undergoing TRUSPB, of which 12 had a preoperative positive urine culture, and detected no difference in the complication rates between the groups. (23) Another study of 150 patients with 6 positive preoperative urine culture found no association between asymptomatic bacteriuria and PBIs. (24)
FORMALIN DIPPING
Dipping the biopsy need in formalin before each individual prostate biopsy is easy and experiments using formalin disinfection show no growth fluoroquinolone resistant organisms and while several studies have shown lower rates of PBI's, the results of these studies have not been statistically significant. (30,31,32)
MRI FUSION BIOPSIES
About 10% of clinically significant lesions not seen on MRI were found with systemic biopsies. (15,16) with two studies finding 16% of men with negative MRI had clinically significant prostate cancer on systemic biopsy. (20,22) A 2020 study found prostate cancer was detected in 79%, 92%, 98% and 100% of cases on the 1st, 2nd, 3rd or 4th biopsy of target lesion. (35) PET FUSION BIOPSY
A prostpective study using PET fusion prostate biopsy showed if a maximum standardized uptake value of 5.4 and maximum-to-background standardized uptake value ratio of 2 had a 100% sensitivity and a 76% specificity for Gleason 7 and 88% for Gleason 6 in the first prospective study for this PET. (21) A meta-analysis and systematic review in 2020 found that the NPV of 90.4% when using a PSAD of 0.15. (36).
SATURATION BIOPSY OF TARGET
A prospective study from 2000-2016 of 208 consecutive patients, including 86 with a saturated and 122 with a nonsaturated lesion. Median age 62.0 years, median PSA 7.1 ng/ml. Median number of biopsy cores per index lesion was 4 in saturated vs 2 in unsaturated. The risk category upgrade rate from systematic only, fusion only, and combined fusion and systematic biopsy results to prostatectomy was 40.9%, 23.6% and 13.8%, respectively. The risk category upgrade from combined fusion and systematic biopsy results was lower in the saturated than in the nonsaturated lesion group (7% vs 18%, p = 0.021). There was no difference in the upgrade rate based on systematic biopsy between the 2 groups. However, fusion biopsy results were significantly less upgraded in the saturated lesion group (Gleason upgrade 20.9% vs 36.9%, p = 0.014 and risk category upgrade 14% vs 30.3%, p = 0.006). The authors concluded the results demonstrated that fusion saturation biopsy of an index lesion (largest and highest PIRADS) b by minimizing the impact of tumor heterogeneity. (2)
NUMBER OF POSITIVE CORES
To help determine whether the number of positive cores should effect active surveillance usage, a retrospective study of 3,359 men with low risk prostate cancer who underwent radical prostatectomy between January 2000 and August 2016 was reviewed. Of the 171 cases (5.1%) with adverse pathology findings at radical prostatectomy 144 (4.3%) were upgraded to Grade Group 3 or greater, 31 (0.9%) had seminal vesicle invasion and 15 (0.4%) had lymph node involvement. Prostate specific antigen and patient age were the only predictors of adverse pathology results. There was no significant association with the number of positive cores, the total mm of cancer or the maximum percent of cancer in any core. When expanding the definition of adverse pathology to include Grade Group 2 and extraprostatic extension, the association between core features and outcome was statistically significant but clinically weak, and with no evidence of threshold effects. There is little basis for excluding patients with otherwise low risk prostate cancer on biopsy from active surveillance based on criteria such as the number of positive cores or the maximum cancer involvement of biopsy cores. (6)
DOWNGRADING
A study of 5,474 Gleason 8 biopsies showed 60% were downgraded on final pathology of post-prostatectomy and this finding is consistent with multiple other studies. (19)
INFLAMMATION ON PROSTATE BIOPSY
A study of 20,585 found inflammation on biopsy associated with OR of 0.455 with prostate cancer. (34)