Stones
Urologists should have low threshold for assessing PTH axis, especially patients w/ high normal CA++ levels and a high normal to increased parathyroid level should raise suspicion for primary hyperthyroidism.
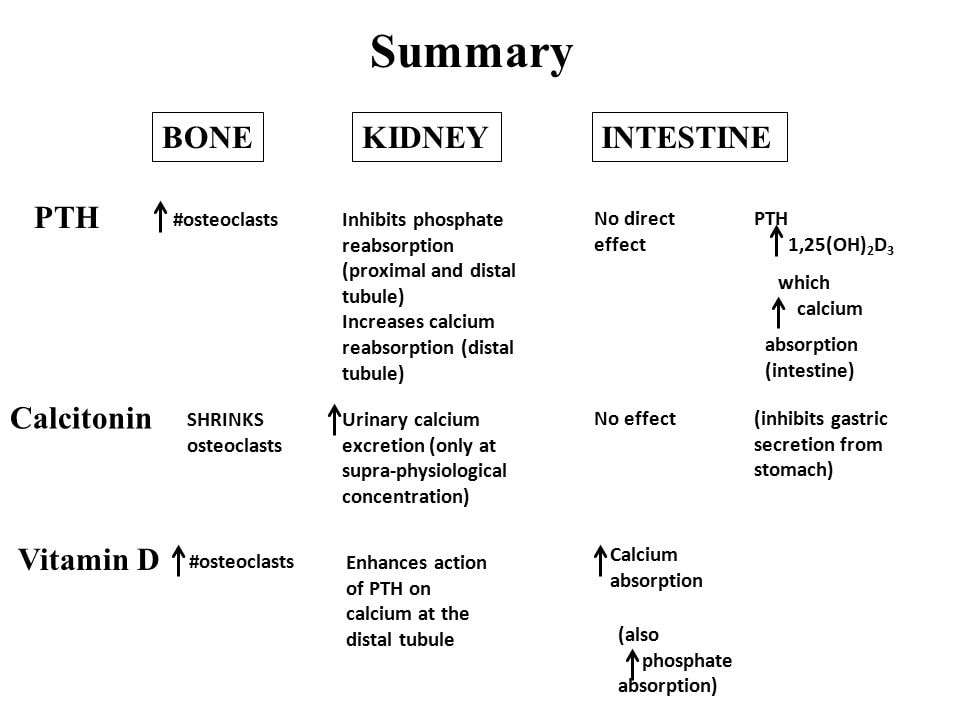
PTH, metabolized by liver, has short 1/2 life (<2 min) and is regulated by ionized Ca++. (1)
VitD converted to 25-OH-VitD in liver, then active form 1,25-OH-VitD in the kidney. 25-OH-Vit D has 1/2 life of 2-3 weeks, reflects storage levels. 1,25-OH-VitD has half life of 6-8 hours. (1) >10,000 units of VitD daily can cause VitD intoxication. 1-alpha hydroxylase is in keratinocytes, placenta and macrophages however is not regulated by normal mechanisms in these cells. 10% of Sarcoidosis patients will have hypercalcemia and 25% will have hypercalciuria (4).
Long term lithium use can cause primary hyperparathyroidism. 10-20% of primary hyperparathyroid patients develop kidney stones and is the most common finding. (2,3) Secondary hyperparathyroidism develops from renal calcium wasting, CKD, bone loss or poor intestinal uptake of Ca++, often due to low VitD. Thiazide challenge for 2 weeks shows elevated PTH if primary hyperparathyroidism and normal PTH with normal Ca if secondary.
65% of calcium stone formers have hypercalciuria. (5) High Ca++ intake (>2000mg/day) is associated with hypercalciuria, low Ca++ intake causes excess oxalate absorption. 1000-1200 mg/day is recommended for Ca++ intake. (6) A High salt diet leads to increased Na+ secretion and reduced calcium reabsopriton int he renal proximal tubule, causing hypercalciuria. (7) High protein diet can cause hypercalciuria in part due to acid load. Corticosteroids and loop diuretics can also lead to hypercalciuria.
STONE TYPES
A case of immunoglobulin free light chain stone in a multiple myeloma patient has been reported. (8)
PTH, metabolized by liver, has short 1/2 life (<2 min) and is regulated by ionized Ca++. (1)
VitD converted to 25-OH-VitD in liver, then active form 1,25-OH-VitD in the kidney. 25-OH-Vit D has 1/2 life of 2-3 weeks, reflects storage levels. 1,25-OH-VitD has half life of 6-8 hours. (1) >10,000 units of VitD daily can cause VitD intoxication. 1-alpha hydroxylase is in keratinocytes, placenta and macrophages however is not regulated by normal mechanisms in these cells. 10% of Sarcoidosis patients will have hypercalcemia and 25% will have hypercalciuria (4).
Long term lithium use can cause primary hyperparathyroidism. 10-20% of primary hyperparathyroid patients develop kidney stones and is the most common finding. (2,3) Secondary hyperparathyroidism develops from renal calcium wasting, CKD, bone loss or poor intestinal uptake of Ca++, often due to low VitD. Thiazide challenge for 2 weeks shows elevated PTH if primary hyperparathyroidism and normal PTH with normal Ca if secondary.
65% of calcium stone formers have hypercalciuria. (5) High Ca++ intake (>2000mg/day) is associated with hypercalciuria, low Ca++ intake causes excess oxalate absorption. 1000-1200 mg/day is recommended for Ca++ intake. (6) A High salt diet leads to increased Na+ secretion and reduced calcium reabsopriton int he renal proximal tubule, causing hypercalciuria. (7) High protein diet can cause hypercalciuria in part due to acid load. Corticosteroids and loop diuretics can also lead to hypercalciuria.
STONE TYPES
A case of immunoglobulin free light chain stone in a multiple myeloma patient has been reported. (8)
- Bringhurst FR, Demay MB and Kronenberg HM: Hormones and Disorders of Mineral Metabolism. In: Williams Textbook of Endocrinology, 13th ed. Edited by S Melmed, KS Polonsky, PR Larsen et al. Philadelphia: Elsevier 2015; p1916.
- Cassibba, Sara, et al. "Silent renal stones in primary hyperparathyroidism: prevalence and clinical features." Endocrine Practice 20.11 (2014): 1137-1142.
- Silverberg, Shonni J., et al. "A 10-year prospective study of primary hyperparathyroidism with or without parathyroid surgery." New England Journal of Medicine 341.17 (1999): 1249-1255.
- 4Rizzato, Gianfranco. "Clinical impact of bone and calcium metabolism changes in sarcoidosis." Thorax 53.5 (1998): 425-429.
- Sakhaee, Khashayar, Naim M. Maalouf, and Bridget Sinnott. "Kidney stones 2012: pathogenesis, diagnosis, and management." The Journal of Clinical Endocrinology & Metabolism 97.6 (2012): 1847-1860.
- Pearle, Margaret S., et al. "Medical management of kidney stones: AUA guideline." The Journal of urology 192.2 (2014): 316-324.
- Ticinesi, Andrea, et al. "Salt and nephrolithiasis." Nephrology Dialysis Transplantation 31.1 (2014): 39-45.
- Bouchet, Antonin, et al. “Acute Renal Colic Due to Immunoglobulin Free Light Chain Kidney Stones: A Case Report of an Unusual Complication of Multiple Myeloma.” American Journal of Kidney Diseases, vol. 74, no. 5, 2019, pp. 700–702.