Varicocelectomy
INDICATIONS
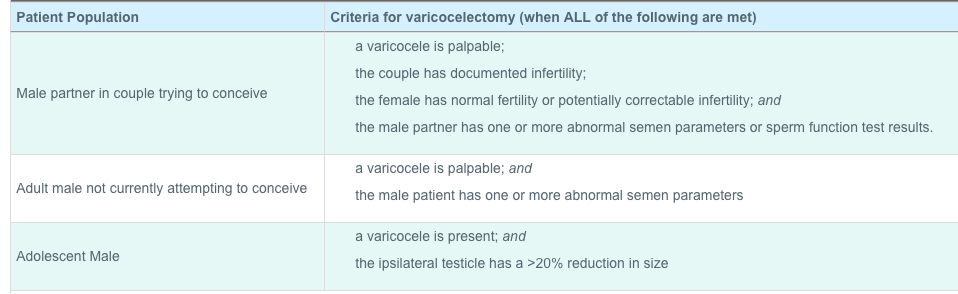
See table below
CONTRAINDICATIONS
BACKGROUND
Left varicocele is more common due to the right angled insertion of the left spermatic vein into the left renal vein. Nutcracker syndrome (L renal vein compressed between SMA and aorta) can cause L varicocele. Varicoceles occur in 15% of males and 40% of males seen in infertility clinic. The majority (75-90%) of varicoceles are left sided, and 33% are bilateral. Varicoceles can cause pain with a dull ache that increases after standing for long periods of time or with activity and improves in the recumbent position is characteristic. See table at bottom of page for indications for surgery
Surgical treatment of varicoceles results in successful correction in greater than 90% of men. Subinguinal, inguinal, and retroperitoneal approaches are used and none has been shown superior yet. (4) A recent study suggests bilateral is superior to unilateral varicoceletomy in infertile males with left clinical and right subclinical varicocele with greater improvements in sperm concentration, normal sperm morphology and progressive motility and spontaneous pregnancy rate after pregnancy. (6)
RISKS
The most common complications of varicocelectomy are hydrocele formation and varicocele recurrence. (5) Microsurgical varicocelectomy have a hydrocele formation rate of <1%, inguinal 3-39% and laparoscopic 5-8%. Microscopic varicocele recurrence rates are 1-2%, non-magnified inguinal 9-16%, high retroperitoneal 11-15%. (1,2,3) Wound infection and hematoma formation reported to likely be very small, <1%. (7) The most feared complication is testicular atrophy or loss from vascular compromise.
KEY POINTS
See table below
CONTRAINDICATIONS
BACKGROUND
Left varicocele is more common due to the right angled insertion of the left spermatic vein into the left renal vein. Nutcracker syndrome (L renal vein compressed between SMA and aorta) can cause L varicocele. Varicoceles occur in 15% of males and 40% of males seen in infertility clinic. The majority (75-90%) of varicoceles are left sided, and 33% are bilateral. Varicoceles can cause pain with a dull ache that increases after standing for long periods of time or with activity and improves in the recumbent position is characteristic. See table at bottom of page for indications for surgery
Surgical treatment of varicoceles results in successful correction in greater than 90% of men. Subinguinal, inguinal, and retroperitoneal approaches are used and none has been shown superior yet. (4) A recent study suggests bilateral is superior to unilateral varicoceletomy in infertile males with left clinical and right subclinical varicocele with greater improvements in sperm concentration, normal sperm morphology and progressive motility and spontaneous pregnancy rate after pregnancy. (6)
RISKS
The most common complications of varicocelectomy are hydrocele formation and varicocele recurrence. (5) Microsurgical varicocelectomy have a hydrocele formation rate of <1%, inguinal 3-39% and laparoscopic 5-8%. Microscopic varicocele recurrence rates are 1-2%, non-magnified inguinal 9-16%, high retroperitoneal 11-15%. (1,2,3) Wound infection and hematoma formation reported to likely be very small, <1%. (7) The most feared complication is testicular atrophy or loss from vascular compromise.
KEY POINTS
- Use a doppler to find the testicular artery, place 2-0 or 4-0 silk under to use to temporarily occlude to ensure preservation during ligation
- Proper identification of the cord in its entirety in order not to leave any dilated veins posteriorly.
- 50% of the time, the testicular artery is adherent to the posterior surface of one of the veins.
- Once all veins have been ligated, the surgeon should perform complete inspection of the field to ensure patency of the testicular artery and ligation of all venous structures.

AUA Core Curriculum 2018
- Schauer, Ingrid, et al. "The impact of varicocelectomy on sperm parameters: a meta-analysis." The Journal of urology187.5 (2012): 1540-1547.
- Ding, Hui, et al. "Open non‐microsurgical, laparoscopic or open microsurgical varicocelectomy for male infertility: a meta‐analysis of randomized controlled trials." BJU international110.10 (2012): 1536-1542.
- Kroese, Anja CJ, et al. "Surgery or embolization for varicoceles in subfertile men." The Cochrane Library (2012).
- Male Infertility Best Practice Policy Committee. Report on varicocele and infertility. American Urological Association. 2001.
- Ding, H., et al., Open non-microsurgical, laparoscopic or open microsurgical varicocelectomy for male infertility: a meta-analysis of randomized controlled trials. BJU Int, 2012. 110(10): p. 1536-42.
- Sun, Xiao-lei, et al. "Bilateral is superior to unilateral varicocelectomy in infertile males with left clinical and right subclinical varicocele: a prospective randomized controlled study." International urology and nephrology 50.2 (2018): 205-210.
- Nguyen HT, Etzell J, Turek PJ. Normal human ejaculatory duct anatomy: a study of cadaveric and surgical specimens. J Urol. May 1996;155(5):1639-1642.