Prostate Cancer Imaging
MRI PROSTATE
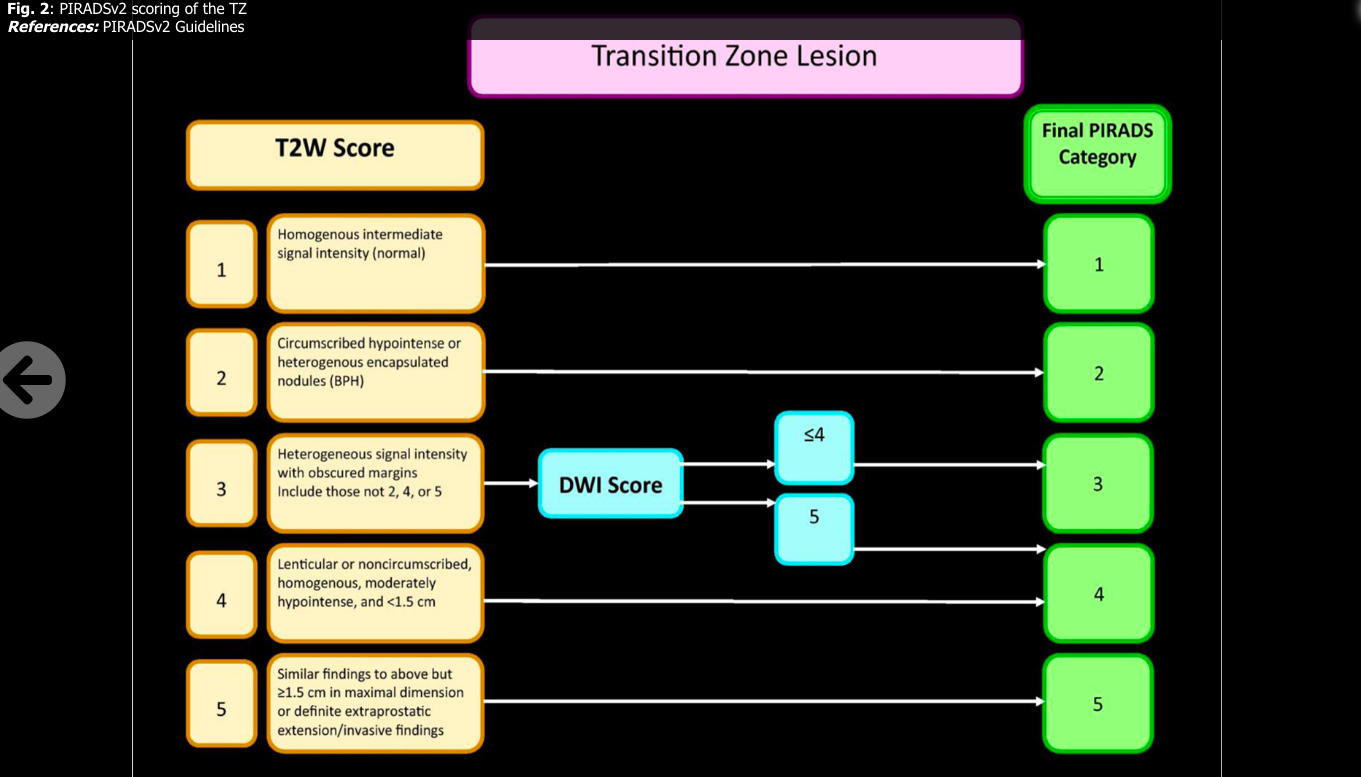
MRI prostate is graded by the PIRADS (prostate imaging reporting and data system), based on PIRADS version 2 (24). There is a scale of 1-5 with PIRADS 4 or 5 needing to be biopsied as PIRADS 4 have ~60% of having Gleason 3+4 or higher and PIRADS 5 having ~90% Gleason 3+4 or higher. PIRADS 1-2 are very low risk for clinically significant prostate cancer and do not get biopsied. PIRADS 3 are more in the grey area regarding the need for biopsy with ~15% rate of clinically significant prostate cancer. One retrospective study of 43 patients showed a 56% rate in PIRADS 3 with 47% GS 3+4 or greater. (5) Another showed 6.5% detection rate and lesions in the TX were more likely to represent benign disease than in the PZ. (6) A retospective study showed gleason 3+3 can develop in PI-RADS 3, 3+4 can also develop and 4+3 is unlikely in PIRADS 3 lesion. If a PSAD of 0.15ng/ml were used as a cutoff in this study, only 0.8% of PCa would not have been detected. These authors promoted follow up MRI of PIRADS3, especially if in the TZ, high prostate volume and PSAD <0.15ng/ml (4)
The PROMIS study of 576 men showed TRUS performs poorly compared to MRI (9) and MRI missed 6-17% of CS-PCA's. (8) Other studies show about 10% of clinically significant lesions not seen on MRI were found with systemic biopsies. (11,12) and a 2015 study of 122 patients found that 28% of patients with Gleason 7 or greater were missed on prostate MRI. (14) Other studies have shown 10% (see here) and up to 16% of men with negative MRI had clinically significant prostate cancer on systemic biopsy. (15) PRECISION study showed MRI with or without targeted biopsy is non-inferior to standard systemic biopsy and more accurate detecting clinically significant disease with fewer cores (20)
The PROMIS study of 576 men showed TRUS performs poorly compared to MRI (9) and MRI missed 6-17% of CS-PCA's. (8) Other studies show about 10% of clinically significant lesions not seen on MRI were found with systemic biopsies. (11,12) and a 2015 study of 122 patients found that 28% of patients with Gleason 7 or greater were missed on prostate MRI. (14) Other studies have shown 10% (see here) and up to 16% of men with negative MRI had clinically significant prostate cancer on systemic biopsy. (15) PRECISION study showed MRI with or without targeted biopsy is non-inferior to standard systemic biopsy and more accurate detecting clinically significant disease with fewer cores (20)
PET
11C-choline and 18F-fluciclovine are the only FDA approved PET tracers for prostate cancer (as of June 2, 2018). They outperform CT, MRI and bone scan, but have limited detection with low levels of PSA. PSMA PET appears to have better detection rates at low PSA.
11C-choline PET
18F-fluciclovine PET
18F-fluciclovine is a synthetic amino acid, first approved for PET in 2016. FALCON study of BCR showed 61% of 85 patients w/ 18F-fluciclovine PET/CT imaging had management changes after this image. Median PSA was 0.63 ng/ml in these men and those with PSA <5 there was a 25% detection rate. Most patients were Gleason 7. (17)
PSMA (Prostate specific membrane antigen) PET
PSMA is overexpressed in CRPC. PSMA PET is the most sensitive for post prostatectomy PSA recurrence to identify mets and primary usage is to identify sites after BCR. 68Ga-PSMA-11 has been used in Europe with a sensitivity of 57% in BCR w/ PSA <1.0. (7) A prospective study using PET fusion prostate biopsy showed if a maximum standardized uptake value of 5.4 and maximum-to-background standardized uptake value ratio of 2 had a 100% sensitivity and a 76% specificity for Gleason 7 and 88% for Gleason 6 in the first prospective study for this PET. (16) However, there appears to be increased uptake in the celiac ganglion compared to other ganglion. For the differentiation between lymph node metastases and sympathetic ganglia, both intensity of 68Ga-PSMA-ligand uptake and exact localization and configuration of the respective lesion should be examined carefully. (18) A 2019 meta-analysis found that in BCR, the detection rate was 0.63 with a PSA of less than 2.0 and 0.94 with a PSA of more than 2.0. (27) A 2020 systematic review and meta-analysis found a detection rate of 50% at PSA of 0.5 to 0.99 ng/ml in BCR. (28)
VERSUS BONE SCAN AND MRI
A retrospective study of 32 PCa patients found PET/MRI was superior to MRI (74% vs 50% sensitivity). (19) A recent study showed 68Ga-PSMA-11 PET localized recurrent prostate cancer in 475 of 635 (75%) patients; detection rates significantly increased with prostate-specific antigen (PSA): 38% for <0.5 ng/mL (n = 136), 57% for 0.5 to <1.0 ng/mL (n = 79), 84% for 1.0 to <2.0 ng/mL (n = 89), 86% for 2.0 to <5.0 ng/mL (n = 158), and 97% for ≥5.0 ng/mL (n = 173, P < .001). (21)
PRIMARY STAGING
One nice prospective study looking at primary staging found in patients with >10% risk of nodal mets on MSKCC with a negative bone scan the sensitivity was 41.5% and specificity of 90.9%. (26) A 2019 meta-analysis of 68Ga-PSMA-11 at initial staging demonstrated a sensitivity of 0.74 and specificity of 0.96 using nodal pathology at prostatectomy as a gold standard. (27)
OTHER STUDIES
One study has found that enzalutamide upregulates PSMA expression and it is possible that this influences the results of PSMA PET in patients with enzalutamide creating the impression of progression that is not accurate. (25) Multiple radiotracers linked to this molecule are also under investigation. Lutetium labeled radionuclides attached to PSMA have also been investigated, showing some PSA and radiographic responses. (2)
VERSUS BONE SCAN AND MRI
A retrospective study of 32 PCa patients found PET/MRI was superior to MRI (74% vs 50% sensitivity). (19) A recent study showed 68Ga-PSMA-11 PET localized recurrent prostate cancer in 475 of 635 (75%) patients; detection rates significantly increased with prostate-specific antigen (PSA): 38% for <0.5 ng/mL (n = 136), 57% for 0.5 to <1.0 ng/mL (n = 79), 84% for 1.0 to <2.0 ng/mL (n = 89), 86% for 2.0 to <5.0 ng/mL (n = 158), and 97% for ≥5.0 ng/mL (n = 173, P < .001). (21)
PRIMARY STAGING
One nice prospective study looking at primary staging found in patients with >10% risk of nodal mets on MSKCC with a negative bone scan the sensitivity was 41.5% and specificity of 90.9%. (26) A 2019 meta-analysis of 68Ga-PSMA-11 at initial staging demonstrated a sensitivity of 0.74 and specificity of 0.96 using nodal pathology at prostatectomy as a gold standard. (27)
OTHER STUDIES
One study has found that enzalutamide upregulates PSMA expression and it is possible that this influences the results of PSMA PET in patients with enzalutamide creating the impression of progression that is not accurate. (25) Multiple radiotracers linked to this molecule are also under investigation. Lutetium labeled radionuclides attached to PSMA have also been investigated, showing some PSA and radiographic responses. (2)
F-DCFPyL PET
ULTRASOUND
Sensitivity and specicity of finding clinically signficiant prostate cancer on TRUS findings were 42% and 91% compared to 62% and 84% of MRI in a retrospective study of 178 men; however, this was biased as 2 highly experienced urologists performed these and had previous knowledge of MRI lesion. 40% of the lesions seen on MRI were also observed on US. This study data suggests biopsing only on MRI or TRUS findings were miss 1/3 of Gleason 3+4 or higher tumors. (8) While that study suggests performing biopsy on lesions seen only on US, the PROMIS findings do not. (9) A 2016 study similarly showed 43% of lesions identified on MRI were visible on TRUS and also these were more likely to represent aggressive tumors that if only seen on MRI. (10)
BONE MET IMAGING
One study found MRI superior to bone scan. (22) One small study found MRI is helpful in the diagnosis of metastatic prostate cancer, especially when other radiographic examinations are inconclusive or spinal cord compression is suspected. (23)
READING PROSTATE MRI
There are 3 key phases to consider with prostate MRI: T2 weighted (T2w), diffusion weighted images (DWI) and dynamic contrast enhanced (DCE). T1w can also help with pelvic MRI in limited situations mentioned below.
T2w
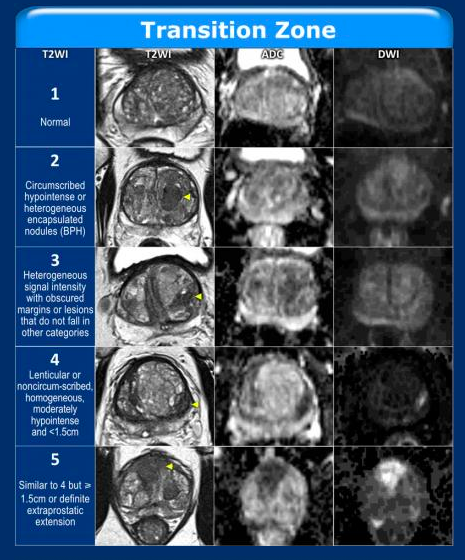
Fluid sensitive with water bright and excellent for anatomy. T2w is key for evaluating lesions in the transition zone and can also identify central zone. BPH are circumscribed with discrete borders and T2w is key for evaluating BPH nodules in the transition zone. Cancers are indistinct with erased boarders.
DWI
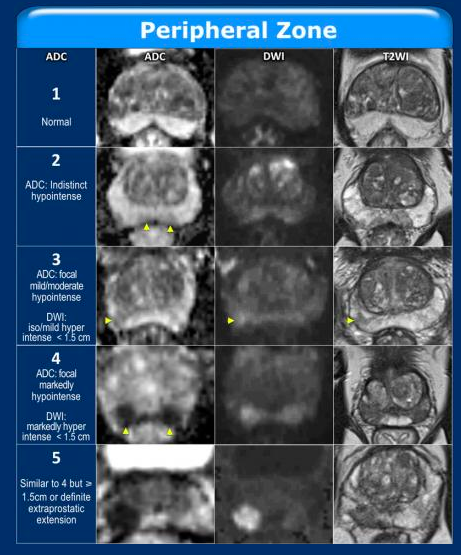
DWI is key for evaluating peripheral zone and give poor anatomic detail. DWI shows random movement of water in tissue which is restricted in cancer. A bright signal on DWI means diffusion is impeded which is found in cancer (but also some other things). A high b-value (strength of gradient for water) is needed for better visualization of DWI (b >1500), however higher b-value does give more background noise. Using the DWI theADC (apparent diffusion coefficient) can be produced and used to simplify multiple diffusion weighted images. If diffusion is truly restricted, this will show up as dark on ADC map.
DCE
This is giving contrast and performing real time MRI to measure enhancement of prostate. If the lesion enhances this means there is blood flow, this can help better characterize suspicious lesions and also help in MRI after radiation. This is useful in equivocal peripheral zone lesion PIRAD3 lesions, if positive can push towards PIRADS 4 lesions.
T1w
Poor for zonal anatomy but good for evaluating bone and lymph nodes and good for identifying hemorrhage and sites of previous biopsy.
T2w
Fluid sensitive with water bright and excellent for anatomy. T2w is key for evaluating lesions in the transition zone and can also identify central zone. BPH are circumscribed with discrete borders and T2w is key for evaluating BPH nodules in the transition zone. Cancers are indistinct with erased boarders.
DWI
DWI is key for evaluating peripheral zone and give poor anatomic detail. DWI shows random movement of water in tissue which is restricted in cancer. A bright signal on DWI means diffusion is impeded which is found in cancer (but also some other things). A high b-value (strength of gradient for water) is needed for better visualization of DWI (b >1500), however higher b-value does give more background noise. Using the DWI theADC (apparent diffusion coefficient) can be produced and used to simplify multiple diffusion weighted images. If diffusion is truly restricted, this will show up as dark on ADC map.
DCE
This is giving contrast and performing real time MRI to measure enhancement of prostate. If the lesion enhances this means there is blood flow, this can help better characterize suspicious lesions and also help in MRI after radiation. This is useful in equivocal peripheral zone lesion PIRAD3 lesions, if positive can push towards PIRADS 4 lesions.
T1w
Poor for zonal anatomy but good for evaluating bone and lymph nodes and good for identifying hemorrhage and sites of previous biopsy.
https://radiologyassistant.nl/abdomen/prostate-cancer-pi-rads-v2
https://radiologyassistant.nl/abdomen/prostate-cancer-pi-rads-v2
Melaki, K., et al. "Transition zone cancer revisited at multiparametric prostate MRI."
Melaki, K., et al. "Transition zone cancer revisited at multiparametric prostate MRI."
- Sobol I, Zaid HB, Haloi R, et al. Contemporary Mapping of Post-Prostatectomy Prostate Cancer Relapse with 11C-Choline Positron Emission Tomography and Multiparametric Magnetic Resonance Imaging. J Urol. 2017;197(1):129-134.
- Rahbar K, Ahmadzadehfar H, Kratochwil C, et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2017;58(1):85-90.
- Gorin, Michael A., et al. "Prostate Specific Membrane Antigen Targeted 18F-DCFPyL Positron Emission Tomography/Computerized Tomography for the Preoperative Staging of High Risk Prostate Cancer: Results of a Prospective, Phase II, Single Center Study." The Journal of urology 199.1 (2018): 126-132.
- Ullrich, Tim, et al. "Risk Stratification of Equivocal Lesions in Multiparametric Magnetic Resonance Imaging of the Prostate." The Journal of urology (2017).
- Washino, Satoshi, et al. "Combination of prostate imaging reporting and data system (PI‐RADS) score and prostate‐specific antigen (PSA) density predicts biopsy outcome in prostate biopsy naïve patients." BJU international 119.2 (2017): 225-233.
- Liddell, Heath, Rajeev Jyoti, and Hodo Z. Haxhimolla. "mp-MRI prostate characterised PIRADS 3 lesions are associated with a low risk of clinically significant prostate cancer-a retrospective review of 92 biopsied PIRADS 3 lesions." Current urology 8.2 (2014): 96-100.
- Afshar-Oromieh, Ali, et al. "Diagnostic performance of 68 Ga-PSMA-11 (HBED-CC) PET/CT in patients with recurrent prostate cancer: evaluation in 1007 patients." European journal of nuclear medicine and molecular imaging 44.8 (2017): 1258-1268.
- Garcia-Reyes, Kirema, et al. "Impact of Lesion Visibility on Transrectal Ultrasound on the Prediction of Clinically Significant Prostate Cancer (Gleason Score 3+ 4 or Greater) with Transrectal Ultrasound-Magnetic Resonance Imaging Fusion Biopsy." The Journal of urology 199.3 (2018): 699-705.
- Ahmed, Hashim U., et al. "Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study." The Lancet389.10071 (2017): 815-822.www.ncbi.nlm.nih.gov/pubmed/28110982.
- van de Ven, Wendy JM, et al. "Visibility of prostate cancer on transrectal ultrasound during fusion with multiparametric magnetic resonance imaging for biopsy." Clinical imaging 40.4 (2016): 745-750.
- Borkowetz, Angelika, et al. "Comparison of systematic transrectal biopsy to transperineal magnetic resonance imaging/ultrasound‐fusion biopsy for the diagnosis of prostate cancer." BJU international 116.6 (2015): 873-879.
- Radtke, Jan Philipp, et al. "The current and future role of magnetic resonance imaging in prostate cancer detection and management." Translational andrology and urology 4.3 (2015): 326.
- Graziani, Tiziano, et al. "11C-Choline PET/CT for restaging prostate cancer. Results from 4,426 scans in a single-centre patient series." European journal of nuclear medicine and molecular imaging 43.11 (2016): 1971-1979.
- Le, Jesse D., et al. "Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: correlation with whole-mount histopathology." European urology 67.3 (2015): 569-576.
- Filson, Christopher P., et al. "Prostate cancer detection with magnetic resonance‐ultrasound fusion biopsy: The role of systematic and targeted biopsies." Cancer 122.6 (2016): 884-892.
- Lopci, Egesta, et al. "68Ga-PSMA Positron Emission Tomography/Computerized Tomography for Primary Diagnosis of Prostate Cancer in Men with Contraindications to or Negative Multiparametric Magnetic Resonance Imaging: A Prospective Observational Study." The Journal of urology200.1 (2018): 95-103.
- Teoh, Eugene Jueren, et al. "The FALCON trial: Impact of 18F-fluciclovine PET/CT on clinical management choices for men with biochemically recurrent prostate cancer." (2018): 165-165.
- Rischpler, Christoph, et al. "68Ga-PSMA-HBED-CC Uptake in Cervical, Celiac, and Sacral Ganglia as an Important Pitfall in Prostate Cancer PET Imaging." Journal of Nuclear Medicine59.9 (2018): 1406-1411.
- Hicks, Robert M., et al. "Diagnostic accuracy of 68Ga-PSMA-11 PET/MRI compared with multiparametric MRI in the detection of prostate cancer." Radiology (2018): 180788.
- Kasivisvanathan, Veeru, et al. "MRI-targeted or standard biopsy for prostate-cancer diagnosis." New England Journal of Medicine 378.19 (2018): 1767-1777.
- Fendler, W. P., Calais, J., Eiber, M., Flavell, R. R., Mishoe, A., Feng, F. Y., … Okamoto, S. (2019). Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncology.
- Ketelsen, D., et al. "Detection of bone metastasis of prostate cancer-comparison of whole-body MRI and bone scintigraphy." RoFo: Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin 180.8 (2008): 746-752.
- Fujii, Y., et al. “Magnetic Resonance Imaging for the Diagnosis of Prostate Cancer Metastatic to Bone.” BJUI, vol. 75, no. 1, 1995, pp. 54–58.
- Weinreb, Jeffrey C., et al. “PI-RADS Prostate Imaging – Reporting and Data System: 2015, Version 2.” European Urology, vol. 69, no. 1, 2016, pp. 16–40.
- Rosar, Florian, et al. “New Insights in the Paradigm of Upregulation of Tumoral PSMA Expression by Androgen Receptor Blockade: Enzalutamide Induces PSMA Upregulation in Castration-Resistant Prostate Cancer Even in Patients Having Previously Progressed on Enzalutamide.” European Journal of Nuclear Medicine and Molecular Imaging, 2020, pp. 1–8.
- Kalmthout, Ludwike W. M. van, et al. “Prospective Validation of Gallium-68 Prostate Specific Membrane Antigen-Positron Emission Tomography/Computerized Tomography for Primary Staging of Prostate Cancer.” The Journal of Urology, vol. 203, no. 3, 2020, pp. 537–545.
- Hope, Thomas A., et al. “Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology.” The Journal of Nuclear Medicine, vol. 60, no. 6, 2019, pp. 786–793.
- Crocerossa, Fabio, et al. "Detection Rate of Prostate Specific Membrane Antigen Tracers for Positron Emission Tomography/Computerized Tomography in Prostate Cancer Biochemical Recurrence: A Systematic Review and Network Meta-Analysis." The Journal of Urology (2020): 10-1097.
MRI
MRI prostate is graded by the PIRADS (prostate imaging reporting and data system), based on PIRADS version 2 (24). There is a scale of 1-5 with PIRADS 4 or 5 needing to be biopsied as PIRADS 4 have ~60% of having Gleason 3+4 or higher and PIRADS 5 having ~90% Gleason 3+4 or higher. PIRADS 1-2 are very low risk for clinically significant prostate cancer and do not get biopsied. PIRADS 3 are more in the grey area regarding the need for biopsy with ~15% rate of clinically significant prostate cancer. One retrospective study of 43 patients showed a 56% rate in PIRADS 3 with 47% GS 3+4 or greater. (5) Another showed 6.5% detection rate and lesions in the TX were more likely to represent benign disease than in the PZ. (6) A retospective study showed gleason 3+3 can develop in PI-RADS 3, 3+4 can also develop and 4+3 is unlikely in PIRADS 3 lesion. If a PSAD of 0.15ng/ml were used as a cutoff in this study, only 0.8% of PCa would not have been detected. These authors promoted follow up MRI of PIRADS3, especially if in the TZ, high prostate volume and PSAD <0.15ng/ml (4)
PET
11C-choline and 18F-fluciclovine are the only FDA approved PET tracers for prostate cancer (as of June 2, 2018). They outperform CT, MRI and bone scan, but have limited detection with low levels of PSA. PSMA PET appears to have better detection rates at low PSA.
11C-choline PET - Using this combined w/ MRI median positive scan is PSA 2.3 for post-prostatectomy biochemical recurrence sites. (1) It is particulary useful at PSA recurrence greater than 1ng/ml. (13) The NCCN and EAU recognize the usefulness of this test.
18F-fluciclovine PET/CT - 18F-fluciclovine is a synthetic amino acid, first approved for PET in 2016. FALCON study of BCR showed 61% of 85 patients w/ 18F-fluciclovine PET/CT imaging had management changes after this image. Median PSA was 0.63 ng/ml in these men and those with PSA <5 there was a 25% detection rate. Most patients were Gleason 7. (17)
PSMA is overexpressed in CRPC. PSMA PET is the most sensitive for post prostatectomy PSA recurrence to identify mets and primary usage is to identify sites after BCR. 68Ga-PSMA-11 has been used in Europe with a sensitivity of 57% in BCR w/ PSA <1.0. (7) A prospective study using PET fusion prostate biopsy showed if a maximum standardized uptake value of 5.4 and maximum-to-background standardized uptake value ratio of 2 had a 100% sensitivity and a 76% specificity for Gleason 7 and 88% for Gleason 6 in the first prospective study for this PET. (16) However, there appears to be increased uptake in the celiac ganglion compared to other ganglion. For the differentiation between lymph node metastases and sympathetic ganglia, both intensity of 68Ga-PSMA-ligand uptake and exact localization and configuration of the respective lesion should be examined carefully. (18) A 2019 meta-analysis found that in BCR, the detection rate was 0.63 with a PSA of less than 2.0 and 0.94 with a PSA of more than 2.0. (27) A 2020 systematic review and meta-analysis found a detection rate of 50% at PSA of 0.5 to 0.99 ng/ml in BCR. (28)
VERSUS BONE SCAN AND MRI
A retrospective study of 32 PCa patients found PET/MRI was superior to MRI (74% vs 50% sensitivity). (19) A recent study showed 68Ga-PSMA-11 PET localized recurrent prostate cancer in 475 of 635 (75%) patients; detection rates significantly increased with prostate-specific antigen (PSA): 38% for <0.5 ng/mL (n = 136), 57% for 0.5 to <1.0 ng/mL (n = 79), 84% for 1.0 to <2.0 ng/mL (n = 89), 86% for 2.0 to <5.0 ng/mL (n = 158), and 97% for ≥5.0 ng/mL (n = 173, P < .001). (21)
PRIMARY STAGING
One nice prospective study looking at primary staging found in patients with >10% risk of nodal mets on MSKCC with a negative bone scan the sensitivity was 41.5% and specificity of 90.9%. (26) A 2019 meta-analysis of 68Ga-PSMA-11 at initial staging demonstrated a sensitivity of 0.74 and specificity of 0.96 using nodal pathology at prostatectomy as a gold standard. (27)
OTHER STUDIES
One study has found that enzalutamide upregulates PSMA expression and it is possible that this influences the results of PSMA PET in patients with enzalutamide creating the impression of progression that is not accurate. (25) Multiple radiotracers linked to this molecule are also under investigation. Lutetium labeled radionuclides attached to PSMA have also been investigated, showing some PSA and radiographic responses. (2)
One study has found that enzalutamide upregulates PSMA expression and it is possible that this influences the results of PSMA PET in patients with enzalutamide. (25)F-DCFPyL PET/CT - 66% sensitivity, 92.7% specificity in a small study (3)
ULTRASOUND
Sensitivity and speficity of finding clinically significant prostate cancer on TRUS findings were 42% and 91% compared to 62% and 84% of MRI in a retrospective study of 178 men; however, this was biased as 2 highly experienced urologists performed these and had previous knowledge of MRI lesion. 40% of the lesions seen on MRI were also observed on US. This study data suggests biopsy only on MRI or TRUS findings were miss 1/3 of Gleason 3+4 or higher tumors. (8) While that study suggests performing biopsy on lesions seen only on US, the PROMIS findings do not. (9) A 2016 study similarly showed 43% of lesions identified on MRI were visible on TRUS and also these were more likely to represent aggressive tumors that if only seen on MRI. (10)
BONE IMAGING
MRI better than bone scan (22)
READING PROSTATE MRI
There are 3 key phases to consider with prostate MRI: T2 weighted (T2w), diffusion weighted images (DWI) and dynamic contrast enhanced (DCE). T1w can also help with pelvic MRI in limited situations mentioned below.
T2w
Fluid sensitive with water bright and excellent for anatomy. T2w is key for evaluating lesions in the transition zone and can also identify central zone. BPH are circumscribed with discrete borders and T2w is key for evaluating BPH nodules in the transition zone. Cancers are indistinct with erased boarders.
DWI
DWI is key for evaluating peripheral zone and give poor anatomic detail. DWI shows random movement of water in tissue which is restricted in acner. A bright signal on DWI means diffusion is impeded which is found in cancer (but also some other things). A high b-value (strength of gradient for water) is needed for better visualization of DWI (b >1500), however higher b-value does give more background noise. Using the DWI theADC (apparent diffusion coefficient) can be produced and used to simplify multiple diffusion weighted images. If diffusion is truly restricted, this will show up as dark on ADC map.
DCE
This is giving contrast and performing real time MRI to measure enhancement of prostate. If the lesion enhances this means there is blood flow, this can help better characterize suspicious lesions and also help in MRI after radiation.
T1w
Poor for zonal anatomy but good for evaluating bone and lymph nodes and good for identifying hemorrhage.
MRI prostate is graded by the PIRADS (prostate imaging reporting and data system), based on PIRADS version 2 (24). There is a scale of 1-5 with PIRADS 4 or 5 needing to be biopsied as PIRADS 4 have ~60% of having Gleason 3+4 or higher and PIRADS 5 having ~90% Gleason 3+4 or higher. PIRADS 1-2 are very low risk for clinically significant prostate cancer and do not get biopsied. PIRADS 3 are more in the grey area regarding the need for biopsy with ~15% rate of clinically significant prostate cancer. One retrospective study of 43 patients showed a 56% rate in PIRADS 3 with 47% GS 3+4 or greater. (5) Another showed 6.5% detection rate and lesions in the TX were more likely to represent benign disease than in the PZ. (6) A retospective study showed gleason 3+3 can develop in PI-RADS 3, 3+4 can also develop and 4+3 is unlikely in PIRADS 3 lesion. If a PSAD of 0.15ng/ml were used as a cutoff in this study, only 0.8% of PCa would not have been detected. These authors promoted follow up MRI of PIRADS3, especially if in the TZ, high prostate volume and PSAD <0.15ng/ml (4)
PET
11C-choline and 18F-fluciclovine are the only FDA approved PET tracers for prostate cancer (as of June 2, 2018). They outperform CT, MRI and bone scan, but have limited detection with low levels of PSA. PSMA PET appears to have better detection rates at low PSA.
11C-choline PET - Using this combined w/ MRI median positive scan is PSA 2.3 for post-prostatectomy biochemical recurrence sites. (1) It is particulary useful at PSA recurrence greater than 1ng/ml. (13) The NCCN and EAU recognize the usefulness of this test.
18F-fluciclovine PET/CT - 18F-fluciclovine is a synthetic amino acid, first approved for PET in 2016. FALCON study of BCR showed 61% of 85 patients w/ 18F-fluciclovine PET/CT imaging had management changes after this image. Median PSA was 0.63 ng/ml in these men and those with PSA <5 there was a 25% detection rate. Most patients were Gleason 7. (17)
PSMA is overexpressed in CRPC. PSMA PET is the most sensitive for post prostatectomy PSA recurrence to identify mets and primary usage is to identify sites after BCR. 68Ga-PSMA-11 has been used in Europe with a sensitivity of 57% in BCR w/ PSA <1.0. (7) A prospective study using PET fusion prostate biopsy showed if a maximum standardized uptake value of 5.4 and maximum-to-background standardized uptake value ratio of 2 had a 100% sensitivity and a 76% specificity for Gleason 7 and 88% for Gleason 6 in the first prospective study for this PET. (16) However, there appears to be increased uptake in the celiac ganglion compared to other ganglion. For the differentiation between lymph node metastases and sympathetic ganglia, both intensity of 68Ga-PSMA-ligand uptake and exact localization and configuration of the respective lesion should be examined carefully. (18) A 2019 meta-analysis found that in BCR, the detection rate was 0.63 with a PSA of less than 2.0 and 0.94 with a PSA of more than 2.0. (27) A 2020 systematic review and meta-analysis found a detection rate of 50% at PSA of 0.5 to 0.99 ng/ml in BCR. (28)
VERSUS BONE SCAN AND MRI
A retrospective study of 32 PCa patients found PET/MRI was superior to MRI (74% vs 50% sensitivity). (19) A recent study showed 68Ga-PSMA-11 PET localized recurrent prostate cancer in 475 of 635 (75%) patients; detection rates significantly increased with prostate-specific antigen (PSA): 38% for <0.5 ng/mL (n = 136), 57% for 0.5 to <1.0 ng/mL (n = 79), 84% for 1.0 to <2.0 ng/mL (n = 89), 86% for 2.0 to <5.0 ng/mL (n = 158), and 97% for ≥5.0 ng/mL (n = 173, P < .001). (21)
PRIMARY STAGING
One nice prospective study looking at primary staging found in patients with >10% risk of nodal mets on MSKCC with a negative bone scan the sensitivity was 41.5% and specificity of 90.9%. (26) A 2019 meta-analysis of 68Ga-PSMA-11 at initial staging demonstrated a sensitivity of 0.74 and specificity of 0.96 using nodal pathology at prostatectomy as a gold standard. (27)
OTHER STUDIES
One study has found that enzalutamide upregulates PSMA expression and it is possible that this influences the results of PSMA PET in patients with enzalutamide creating the impression of progression that is not accurate. (25) Multiple radiotracers linked to this molecule are also under investigation. Lutetium labeled radionuclides attached to PSMA have also been investigated, showing some PSA and radiographic responses. (2)
One study has found that enzalutamide upregulates PSMA expression and it is possible that this influences the results of PSMA PET in patients with enzalutamide. (25)F-DCFPyL PET/CT - 66% sensitivity, 92.7% specificity in a small study (3)
ULTRASOUND
Sensitivity and speficity of finding clinically significant prostate cancer on TRUS findings were 42% and 91% compared to 62% and 84% of MRI in a retrospective study of 178 men; however, this was biased as 2 highly experienced urologists performed these and had previous knowledge of MRI lesion. 40% of the lesions seen on MRI were also observed on US. This study data suggests biopsy only on MRI or TRUS findings were miss 1/3 of Gleason 3+4 or higher tumors. (8) While that study suggests performing biopsy on lesions seen only on US, the PROMIS findings do not. (9) A 2016 study similarly showed 43% of lesions identified on MRI were visible on TRUS and also these were more likely to represent aggressive tumors that if only seen on MRI. (10)
BONE IMAGING
MRI better than bone scan (22)
READING PROSTATE MRI
There are 3 key phases to consider with prostate MRI: T2 weighted (T2w), diffusion weighted images (DWI) and dynamic contrast enhanced (DCE). T1w can also help with pelvic MRI in limited situations mentioned below.
T2w
Fluid sensitive with water bright and excellent for anatomy. T2w is key for evaluating lesions in the transition zone and can also identify central zone. BPH are circumscribed with discrete borders and T2w is key for evaluating BPH nodules in the transition zone. Cancers are indistinct with erased boarders.
DWI
DWI is key for evaluating peripheral zone and give poor anatomic detail. DWI shows random movement of water in tissue which is restricted in acner. A bright signal on DWI means diffusion is impeded which is found in cancer (but also some other things). A high b-value (strength of gradient for water) is needed for better visualization of DWI (b >1500), however higher b-value does give more background noise. Using the DWI theADC (apparent diffusion coefficient) can be produced and used to simplify multiple diffusion weighted images. If diffusion is truly restricted, this will show up as dark on ADC map.
DCE
This is giving contrast and performing real time MRI to measure enhancement of prostate. If the lesion enhances this means there is blood flow, this can help better characterize suspicious lesions and also help in MRI after radiation.
T1w
Poor for zonal anatomy but good for evaluating bone and lymph nodes and good for identifying hemorrhage.