Non Muscle Invasive Bladder Cancer
Bladder cancer is the 9th most expensive malignancy to treat and has the highest recurrence rate of all solid malignancies. (6)
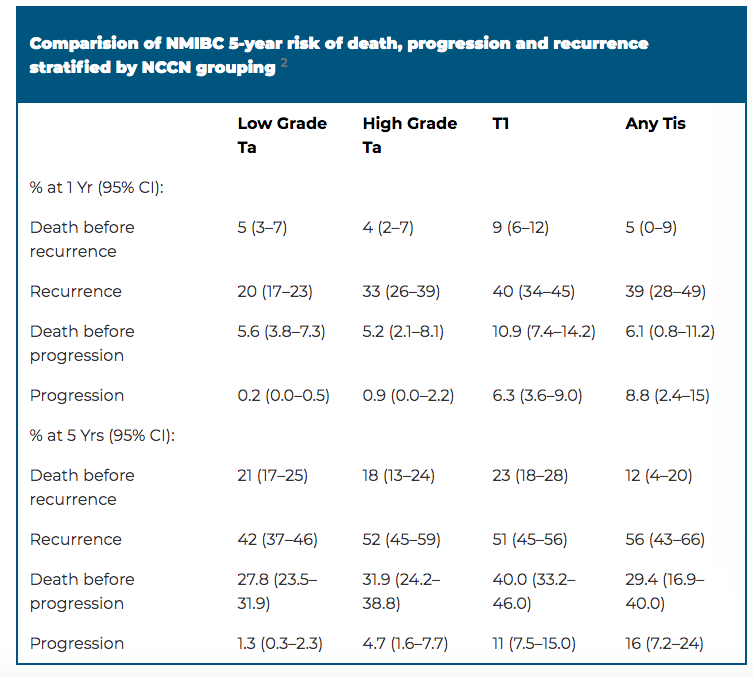
Cancer-specific survival (CSS) in high-grade disease ranges from approximately 70-85% at 10 years and a much higher rate for low-grade disease. (2,3) Low-grade Ta have a recurrence rate of approximately 55%, with ~6% showing stage progression with the 5 yrear progression rate of LG Ta of 0.8%. (3,4) HG T1 lesions have recurrence rate of 45% and progression rate of 17%. (1) 5% of bladder cancer has upper tract tumor involvement. (3)
1yr progression rate is 7.9%, 1.2% and 0.3% for high, intermediate and low risk AUA/SUO NMIBC risk model of recurrence.(8)
REPEAT TURBT
One study of patients with T1 tumors found 82% of patients with residual tumor on repeat TURBT progressed to MIBC within 5 years versus 19% of patients with no residual tumor on repeat TURBT. (10)
EORTC risk calculator combined data from 7 studies, however did not have BCG, intravesical chemo or restaging TURBT. (5)
RESISTANT TO BCG
Targeting IL-15 has been fast tracked by the FDA for treating BCG resistant NMIBC. (9)
Cancer-specific survival (CSS) in high-grade disease ranges from approximately 70-85% at 10 years and a much higher rate for low-grade disease. (2,3) Low-grade Ta have a recurrence rate of approximately 55%, with ~6% showing stage progression with the 5 yrear progression rate of LG Ta of 0.8%. (3,4) HG T1 lesions have recurrence rate of 45% and progression rate of 17%. (1) 5% of bladder cancer has upper tract tumor involvement. (3)
1yr progression rate is 7.9%, 1.2% and 0.3% for high, intermediate and low risk AUA/SUO NMIBC risk model of recurrence.(8)
REPEAT TURBT
One study of patients with T1 tumors found 82% of patients with residual tumor on repeat TURBT progressed to MIBC within 5 years versus 19% of patients with no residual tumor on repeat TURBT. (10)
EORTC risk calculator combined data from 7 studies, however did not have BCG, intravesical chemo or restaging TURBT. (5)
RESISTANT TO BCG
Targeting IL-15 has been fast tracked by the FDA for treating BCG resistant NMIBC. (9)
(7) Downs, Tracy M., et al. “Can We Improve Nonmuscle Invasive Bladder Cancer Guideline Adherence With Smarter Risk Stratification.” The Journal of Urology, vol. 200, no. 4, 2018, pp. 706–708.
Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Joint Guideline (1)
- Palou J, Sylvester RJ, Faba OR et al: Female gender and carcinoma in situ in the prostatic urethra are prognostic factors for recurrence, progression, and disease-specific mortality in T1G3 bladder cancer patients treated with bacillus Calmette-Guerin. Eur Urol 2012;62:118.
- Cookson MS, Herr HW, Zhang ZF et al: The treated natural history of high risk superficial bladder cancer: 15-year outcome. J Urol 1997; 158:62.
- Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Joint Guideline
- Leblanc B, Duclos AJ, Benard F et al: Long-term followup of initial Ta grade 1 transitional cell carcinoma of the bladder. J Urol 1999; 162:1946.
- Sylvester RJ, van der Meijden AP, Oosterlinck W et al: Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol 2006;49:466.
- Loras, A., et al. "Bladder cancer recurrence surveillance by urine metabolomics analysis." Scientific reports 8.1 (2018): 9172.
- Downs, Tracy M., et al. “Can We Improve Nonmuscle Invasive Bladder Cancer Guideline Adherence With Smarter Risk Stratification.” The Journal of Urology, vol. 200, no. 4, 2018, pp. 706–708.
- Ravvaz, Kourosh, et al. “American Urological Association Nonmuscle Invasive Bladder Cancer Risk Model Validation—Should Patient Age Be Added to the Risk Model?” The Journal of Urology, vol. 202, no. 4, 2019, p. 101097.
- Knudson, Karin M., et al. “Mechanisms Involved in IL-15 Superagonist Enhancement of Anti-PD-L1 Therapy.” Journal for ImmunoTherapy of Cancer, vol. 7, no. 1, 2019, p. 82.
- Herr, Harry W., S. Machele Donat, and Guido Dalbagni. "Can restaging transurethral resection of T1 bladder cancer select patients for immediate cystectomy?." The Journal of urology 177.1 (2007): 75-79.