CYSTECTOMY
For Cystectomy high yield intraoperative points click here.
OPERATIVE RISKS
60% of patients experience some complication. (6,7,8,16,17). Death rate of <5% has been observed in cystectomy (17) but may increase to over 10% in patients > 75 years of age and almost 20% in octagenarians. (18) Cardiovascular risk is very high as well, one study looked at continuing antiplatelet therapy during surgery with interesting results. (25)
VTE
VTE are one of the most common occurring in between 2.9% (low risk) to 11.6% (high risk) in open cystectomy (3,036 patients) and rates of 2.6% (low risk) to 10.3% (high risk) in robotic cystectomy (1,320) with majority after discharge from hospital. These rates may be even higher after neoadjuvant chemotherapy with one study of 42 patients showing 19% rate after NAC (21) and another showing 14%. (23) 28 days of prophylaxis are recommended and there is an increase in bleeding with a 0.3% operative re-intervention rate that usually occurs within 7 days post operatively but a 55-60% RR reduction of VTE with extended prophylaxis. Using tinazparin is safer if CrCl <20ml/min. (21)
ROBOTIC vs. OPEN
RCT of 302 patients showed at 2 years similar oncologic outcomes, reduced transfusion, reduced hospital stay. (15) Cystectomy has considerable morbidity, including gastrointestinal, genitourinary, infectious and wound-related complications totaling over 60% within 90 days of surgery, even in high-volume centers of excellence and regardless of open versus robotic approaches (6,16,17)
HEMODIALYSIS PATIENTS
Patients on HD have very bad outcomes after radical cystectomy (RC) . In a retrospective study of 985 patients on HD who underwent RC, Median hospital length of stay was 10 days and 43.1% of patients experienced a complication. Mortality within 30 days was 9.3%. Overall mortality at 1, 3, and 5 years was 51.7%, 77.3%, and 87.9%, respectively. Cancer-specific mortality at 1, 3, and 5 years was 12.3%, 18.4%, and 19.7%, respectively. Age, diabetes, and cerebrovascular disease were independently associated with overall mortality, while performance of urinary diversion was associated with a protective effect. Active smoking was the sole risk factor for cancer-specific mortality. RC in dialysis patients is associated with significant morbidity and mortality, with less than 15% overall survival at 5 years. Older patients, and those with a history of diabetes or cerebrovascular disease, are at an increased risk of mortality. (1)
AGE
A retrospective study in 2017 found patients greater than 75 years old treated with cystectomy for MIBC have a survival advantage and age alone is not the best criteria for surgical candidates, rather frailty or comorbidity criteria. (2) Another study of advanced age in 2017 look at 40 patients over 80 w/ MIBC treated with trimodal therapy showed 54.9% OS at 3 yrs, which is comparable with radical cystectomy. RFS 42.3% at 3 years. 77% of these 40 were treated this due to underlying comorbities and 10% was for patient preference. (3) Death rate of <5% has been observed in cystectomy (17) but may increase to over 10% in patients > 75 years of age and almost 20% in octagenarians. (18)
UPPER TRACT RECURRENCE AND PREOPERATIVE STENTING
A Swiss retrospective study of 1,005 patients with bladder cancer who underwent radical cystectomy between 2000 and 2016 found that preoperative drainage of the upper urinary tract was performed in 114 of the 1,005 patients (11%), including in 53 (46%) by Double-J® stenting and in 61 (54%) by percutaneous nephrostomy. Recurrence developed in the upper urinary tract in 31 patients (3%) at a median of 17 months after cystectomy, including 7 of 53 (13%) in the Double-J group, 0% in the nephrostomy group and 24 of 891 (3%) in the no drainage group. Multivariate regression analysis revealed a higher risk of upper urinary tract recurrence if patients underwent Double-J stenting (HR 4.54, 95% CI 1.43–14.38, p = 0.01) and preoperative intravesical instillations (HR 2.94, 95% CI 1.40–6.16, p = 0.004). (4) It is worth noting 39 of the 53 patients who had a stent recieved this intraoperatively with TURBT and occurred with resection of the ureteral orifice, which is an risk factor itself for recurrence . (4,22)
BACTERURIA
Up to 50% of diversions have E. coli or enterocci w/o signs of infection and more than 75% of patients with diversions have bacteruria present. Inflammatory indices were materially different than the response found with bacteria in the bladder. (12)
PARASTOMAL HERNIA (PSH)
Study of 383 patients who underwent robot assisted radical cystectomy and ileal conduit showed 20% had a parastomal hernia, with 31% of those symptomatic and 15% undergoing treatment with a median time to occurance of 13months. Other studies report a PSH rate of 5% to 65%. (14)
URINARY TRACT INFECTIONS POST-CYSTECTOMY
Prophylactic post-operative antibiotics have been shown to reduce post operative infections with 10-40% of patients getting UTI. These most commonly occur at 3 weeks post operative around the stent removal time. (19) A study published in 2021 found that not using stents decreased complication rate. (26)
URETEROENTERIC STRICTURES
One study found 12, 16 and 19% stricture rate at 1, 3 and 5 years. (20) Ureteral stricture is common with one study of 553 patients reviewed ureteral stricture developed in 7% with a mean followup of 20.2 months (range 1 to 98). Strictures developed in 11% of the orthotopic ileal neobladder, 2.5% of ileal conduit and 8% of Indiana pouch cases. Open repair led to an overall success rate of 87%. (10) One study found using ICG reduced the amount of ureteroenteric strictures in robotic cases (0 vs. 10.6%). (24) A study published in 2021 found that not using stents decreased complication rate. (26)
FISTULA
3.0% or less fistula rate from several studies with a mean 31 days from one large retrospective study. (5,6,9,10,11) No patient had recurrence after surgical repair of the fistula in one study (10) and another study had 100% success rates with 41% not require surgery and only 3% (1 patient) requiring surgery more than once. (5) 10% of fistulas can be seen with cystoscopy (13)
RENAL FAILURE / IMPAIREMENT
One large study showed estimated that more than 16% of patients experienced renal failure or impairment after urinary diversion with renal failure more common after conduit vs. continent diversion. (11)
PELVIC LYMPH NODE DISSECTION
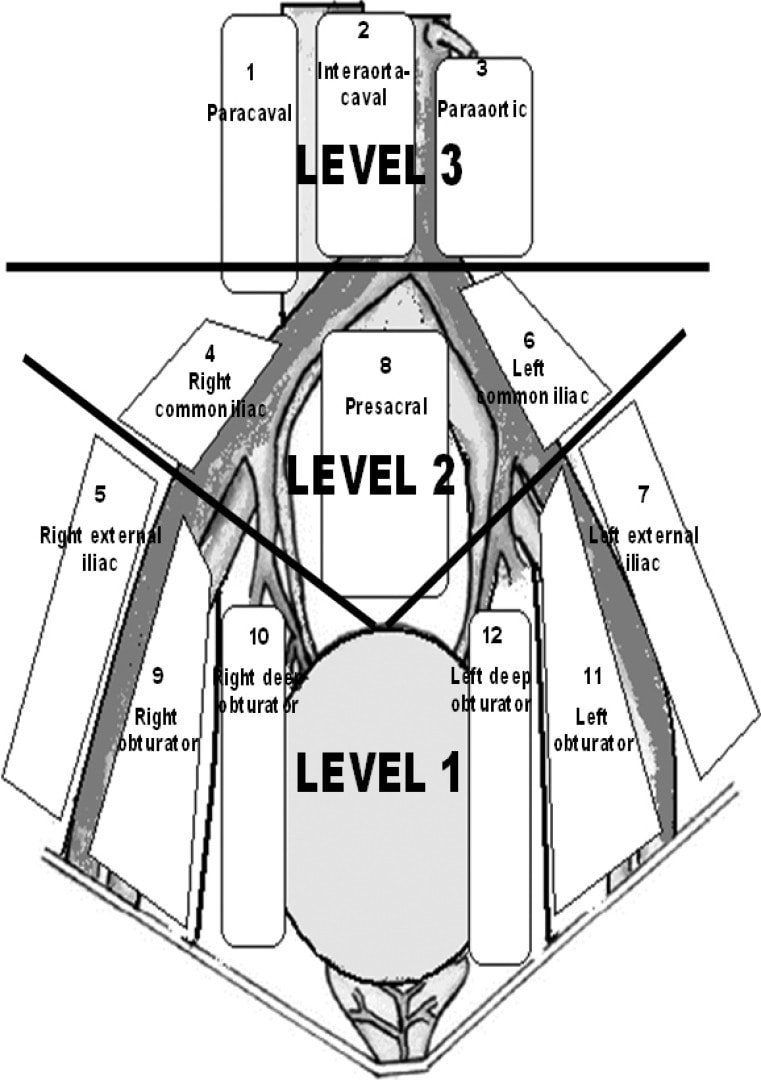
STANDARD BOUNDARIES (LEVEL 1)
Proximal: bifurcation of common iliac
Lateral: genitofemoral nerve to include obturator fossa
Inferior: internal iliac lymph nodes, floor of pelvis
Posterior: sacrum
EXTENDED BOUNDARIES (LEVEL 2)
Proximal: bifurcation of aorta, others same as above
SUPEREXTENDED BOUNDARIES (LEVEL 3)
Proximal: Aorta at the origin of the IMA
OPERATIVE RISKS
60% of patients experience some complication. (6,7,8,16,17). Death rate of <5% has been observed in cystectomy (17) but may increase to over 10% in patients > 75 years of age and almost 20% in octagenarians. (18) Cardiovascular risk is very high as well, one study looked at continuing antiplatelet therapy during surgery with interesting results. (25)
VTE
VTE are one of the most common occurring in between 2.9% (low risk) to 11.6% (high risk) in open cystectomy (3,036 patients) and rates of 2.6% (low risk) to 10.3% (high risk) in robotic cystectomy (1,320) with majority after discharge from hospital. These rates may be even higher after neoadjuvant chemotherapy with one study of 42 patients showing 19% rate after NAC (21) and another showing 14%. (23) 28 days of prophylaxis are recommended and there is an increase in bleeding with a 0.3% operative re-intervention rate that usually occurs within 7 days post operatively but a 55-60% RR reduction of VTE with extended prophylaxis. Using tinazparin is safer if CrCl <20ml/min. (21)
ROBOTIC vs. OPEN
RCT of 302 patients showed at 2 years similar oncologic outcomes, reduced transfusion, reduced hospital stay. (15) Cystectomy has considerable morbidity, including gastrointestinal, genitourinary, infectious and wound-related complications totaling over 60% within 90 days of surgery, even in high-volume centers of excellence and regardless of open versus robotic approaches (6,16,17)
HEMODIALYSIS PATIENTS
Patients on HD have very bad outcomes after radical cystectomy (RC) . In a retrospective study of 985 patients on HD who underwent RC, Median hospital length of stay was 10 days and 43.1% of patients experienced a complication. Mortality within 30 days was 9.3%. Overall mortality at 1, 3, and 5 years was 51.7%, 77.3%, and 87.9%, respectively. Cancer-specific mortality at 1, 3, and 5 years was 12.3%, 18.4%, and 19.7%, respectively. Age, diabetes, and cerebrovascular disease were independently associated with overall mortality, while performance of urinary diversion was associated with a protective effect. Active smoking was the sole risk factor for cancer-specific mortality. RC in dialysis patients is associated with significant morbidity and mortality, with less than 15% overall survival at 5 years. Older patients, and those with a history of diabetes or cerebrovascular disease, are at an increased risk of mortality. (1)
AGE
A retrospective study in 2017 found patients greater than 75 years old treated with cystectomy for MIBC have a survival advantage and age alone is not the best criteria for surgical candidates, rather frailty or comorbidity criteria. (2) Another study of advanced age in 2017 look at 40 patients over 80 w/ MIBC treated with trimodal therapy showed 54.9% OS at 3 yrs, which is comparable with radical cystectomy. RFS 42.3% at 3 years. 77% of these 40 were treated this due to underlying comorbities and 10% was for patient preference. (3) Death rate of <5% has been observed in cystectomy (17) but may increase to over 10% in patients > 75 years of age and almost 20% in octagenarians. (18)
UPPER TRACT RECURRENCE AND PREOPERATIVE STENTING
A Swiss retrospective study of 1,005 patients with bladder cancer who underwent radical cystectomy between 2000 and 2016 found that preoperative drainage of the upper urinary tract was performed in 114 of the 1,005 patients (11%), including in 53 (46%) by Double-J® stenting and in 61 (54%) by percutaneous nephrostomy. Recurrence developed in the upper urinary tract in 31 patients (3%) at a median of 17 months after cystectomy, including 7 of 53 (13%) in the Double-J group, 0% in the nephrostomy group and 24 of 891 (3%) in the no drainage group. Multivariate regression analysis revealed a higher risk of upper urinary tract recurrence if patients underwent Double-J stenting (HR 4.54, 95% CI 1.43–14.38, p = 0.01) and preoperative intravesical instillations (HR 2.94, 95% CI 1.40–6.16, p = 0.004). (4) It is worth noting 39 of the 53 patients who had a stent recieved this intraoperatively with TURBT and occurred with resection of the ureteral orifice, which is an risk factor itself for recurrence . (4,22)
BACTERURIA
Up to 50% of diversions have E. coli or enterocci w/o signs of infection and more than 75% of patients with diversions have bacteruria present. Inflammatory indices were materially different than the response found with bacteria in the bladder. (12)
PARASTOMAL HERNIA (PSH)
Study of 383 patients who underwent robot assisted radical cystectomy and ileal conduit showed 20% had a parastomal hernia, with 31% of those symptomatic and 15% undergoing treatment with a median time to occurance of 13months. Other studies report a PSH rate of 5% to 65%. (14)
URINARY TRACT INFECTIONS POST-CYSTECTOMY
Prophylactic post-operative antibiotics have been shown to reduce post operative infections with 10-40% of patients getting UTI. These most commonly occur at 3 weeks post operative around the stent removal time. (19) A study published in 2021 found that not using stents decreased complication rate. (26)
URETEROENTERIC STRICTURES
One study found 12, 16 and 19% stricture rate at 1, 3 and 5 years. (20) Ureteral stricture is common with one study of 553 patients reviewed ureteral stricture developed in 7% with a mean followup of 20.2 months (range 1 to 98). Strictures developed in 11% of the orthotopic ileal neobladder, 2.5% of ileal conduit and 8% of Indiana pouch cases. Open repair led to an overall success rate of 87%. (10) One study found using ICG reduced the amount of ureteroenteric strictures in robotic cases (0 vs. 10.6%). (24) A study published in 2021 found that not using stents decreased complication rate. (26)
FISTULA
3.0% or less fistula rate from several studies with a mean 31 days from one large retrospective study. (5,6,9,10,11) No patient had recurrence after surgical repair of the fistula in one study (10) and another study had 100% success rates with 41% not require surgery and only 3% (1 patient) requiring surgery more than once. (5) 10% of fistulas can be seen with cystoscopy (13)
RENAL FAILURE / IMPAIREMENT
One large study showed estimated that more than 16% of patients experienced renal failure or impairment after urinary diversion with renal failure more common after conduit vs. continent diversion. (11)
PELVIC LYMPH NODE DISSECTION
STANDARD BOUNDARIES (LEVEL 1)
Proximal: bifurcation of common iliac
Lateral: genitofemoral nerve to include obturator fossa
Inferior: internal iliac lymph nodes, floor of pelvis
Posterior: sacrum
EXTENDED BOUNDARIES (LEVEL 2)
Proximal: bifurcation of aorta, others same as above
SUPEREXTENDED BOUNDARIES (LEVEL 3)
Proximal: Aorta at the origin of the IMA
Ozen, Haluk, et al. "Extended pelvic lymph node dissection: before or after radical cystectomy? A multicenter study of the Turkish society of urooncology." Korean journal of urology 53.7 (2012): 451-456.
- Johnson, Scott, et al. "MP04-16 PERIOPERATIVE AND LONG TERM OUTCOMES AFTER RADICAL CYSTECTOMY IN HEMODIALYSIS PATIENTS." The Journal of Urology 197.4 (2017): e34-e35.
- Bream, Matthew J., et al. "Increased use of cystectomy in patients 75 and older: a contemporary analysis of survival and perioperative outcomes from the National Cancer Database." Urology 100 (2017): 72-78.
- McPherson, Victor A., et al. "Chemoradiotherapy in octogenarians as primary treatment for muscle-invasive bladder cancer." Canadian Urological Association Journal11.1-2 (2017): 24.
- Kiss, Bernhard, et al. "Stenting Prior to Cystectomy is an Independent Risk Factor for Upper Urinary Tract Recurrence." The Journal of urology 198.6 (2017): 1263-1268.
- Smith, Zachary L., et al. "Fistulous complications following radical cystectomy for bladder cancer: analysis of a large modern cohort." The Journal of urology 199.3 (2018): 663-668.
- Shabsigh, Ahmad, et al. "Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology." European urology 55.1 (2009
- Daneshmand, Siamak, et al. "Enhanced recovery protocol after radical cystectomy for bladder cancer." The Journal of urology 192.1 (2014): 50-56.
- Hautmann, Richard E., Robert C. de Petriconi, and Bjoern G. Volkmer. "Lessons learned from 1,000 neobladders: the 90-day complication rate." The Journal of urology 184.3 (2010): 990-994.
- Kim, Simon P., et al. "Contemporary trends of in‐hospital complications and mortality for radical cystectomy." BJU international 110.8 (2012): 1163-1168.
- Msezane, Lambda, et al. "Open surgical repair of ureteral strictures and fistulas following radical cystectomy and urinary diversion." The Journal of urology 179.4 (2008): 1428-1431.
- Gilbert, Scott M., et al. "Downstream complications following urinary diversion." The Journal of urology 190.3 (2013): 916-922.
- Suriano, Francesca, et al. "Bacteriuria in patients with an orthotopic ileal neobladder: urinary tract infection or asymptomatic bacteriuria?." BJU international 101.12 (2008): 1576-1579.
- Melchior, Sebastian, et al. "Diagnosis and surgical management of colovesical fistulas due to sigmoid diverticulitis." The Journal of urology 182.3 (2009): 978-982.
- Hussein, Ahmed A., et al. "Natural history and predictors of parastomal hernia after robot-assisted radical cystectomy and ileal conduit urinary diversion." The Journal of urology 199.3 (2018): 766-773.
- Parekh, Dipen J., et al. "Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): an open-label, randomised, phase 3, non-inferiority trial." The Lancet 391.10139 (2018): 2525-2536.
- Stein JP, Lieskovsky G, Cote R et al: Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol 2001; 19: 666.
- AUA Guidelines: NMIBC. Accessed 10/26/18
- Bochner BH, Dalbagni G, Sjoberg DD et al: Comparing open radical cystectomy and robot-assisted laparoscopic radical cystectomy: a randomized clinical trial. Eur Urol 2015;67:1042.
- Werntz, Ryan P., et al. “Prophylactic Antibiotics Following Radical Cystectomy Reduces Urinary Tract Infections and Readmission for Sepsis from a Urinary Source.” Urologic Oncology-Seminars and Original Investigations, vol. 36, no. 5, 2018.
- Ahmed, Youssef E., et al. “Natural History, Predictors and Management of Ureteroenteric Strictures after Robot Assisted Radical Cystectomy.” The Journal of Urology, vol. 198, no. 3, 2017, pp. 567–574.
- Klaassen, Zachary W. A., et al. “Extended Venous Thromboembolism Prophylaxis after Radical Cystectomy: A Call for Adherence to Current Guidelines.” The Journal of Urology, vol. 199, no. 4, 2017, pp. 906–914.
- Palou, Joan, et al. “Upper Tract Urothelial Tumor after Transurethral Resection for Bladder Tumor.” European Urology, vol. 21, no. 2, 1992, pp. 110–114.
- Duivenvoorden, Wilhelmina C. M., et al. “Incidence, Characteristics and Implications of Thromboembolic Events in Patients with Muscle Invasive Urothelial Carcinoma of the Bladder Undergoing Neoadjuvant Chemotherapy.” The Journal of Urology, vol. 196, no. 6, 2016, pp. 1627–1633.
- Ahmadi, Nariman, et al. "Use of indocyanine green to minimise uretero‐enteric strictures after robotic radical cystectomy." BJU international 124.2 (2019): 302-307.
- Wessels, F., et al. "Radical cystectomy under continuous antiplatelet therapy with acetylsalicylic acid." European Journal of Surgical Oncology 45.7 (2019): 1260-1265.
- Donat, Sherri M., et al. "Intraoperative ureteral stent use at radical cystectomy is associated with higher 30-day complication rates." The Journal of Urology 205.2 (2021): 483-490.